ņä£ ļĪĀ
ņŗĀņāØņĢä 1000ļ¬ģ ņżæ 1-3ļ¬ģņØĆ ņśüĻĄ¼ņĀüņØĖ ļé£ņ▓ŁņØä Ļ░Ćņ¦ĆĻ│Ā Ēā£ņ¢┤ļé£ļŗż[1,2]. ņŗĀņāØņĢäņØś ņśüĻĄ¼ņĀü ļé£ņ▓ŁņØĆ ĻĄ¼ņ¢┤ ņØśņé¼ņåīĒåĄ ļŖźļĀźņØä ņĀĆĒĢśņŗ£ĒéżĻ│Ā ņČöĒøä ĒĢÖņŖĄĻ│╝ ņé¼ĒÜīņĀü ĒÖ£ļÅÖņØś ņןņĢĀļź╝ ņ┤łļלĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņśüĻĄ¼ņĀü ļé£ņ▓ŁņØä Ļ░Ćņ¦ĆĻ│Ā Ēā£ņ¢┤ļéśļŹöļØ╝ļÅä ņĪ░ĻĖ░ņŚÉ ņ▓ŁĻ░ü ņ×¼ĒÖ£ņØä ļ░øņ£╝ļ®┤ ņĀĢņāüņŚÉ Ļ░ĆĻ╣īņÜ┤ ĻĄ¼ņ¢┤ ņØśņé¼ņåīĒåĄ ļŖźļĀźņØä ņŖĄļōØĒĢĀ ņłś ņ׳ļŗż. ņäĀņ▓£ņä▒ ļé£ņ▓Ł ņĢäļÅÖņØś ņĪ░ĻĖ░ ņ▓ŁĻ░ü ņ×¼ĒÖ£ņØä ņ£äĒĢ┤ ļ¬©ļōĀ ņŗĀņāØņĢäļź╝ ļīĆņāüņ£╝ļĪ£ ņŗĀņāØņĢä ņ▓ŁĻ░üņäĀļ│äĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļ®░ ņØ┤ļź╝ ĒåĄĻ│╝ĒĢśņ¦Ć ļ¬╗ĒĢĀ Ļ▓ĮņÜ░ ņāØĒøä 3Ļ░£ņøö ņØ┤ļé┤ņŚÉ ļé£ņ▓Ł ĒÖĢņ¦äņØä ņ£äĒĢ£ ņĀĢļ░Ć ņ▓ŁļĀźĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśĻ│Ā, ļé£ņ▓ŁņØ┤ ĒÖĢņ¦äļÉśļ®┤ ņāØĒøä 6Ļ░£ņøö ņØ┤ļé┤ņŚÉ ļ│┤ņ▓ŁĻĖ░ļź╝ ņØ┤ņÜ®ĒĢ£ ņ▓ŁĻ░ü ņ×¼ĒÖ£ņØä ņŗ£ņ×æĒĢ£ļŗż. Ļ│ĀļÅä Ēś╣ņØĆ ņŗ¼ļÅä Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ ļé£ņ▓Łņ£╝ļĪ£ ļ¦É-ņ¢Ėņ¢┤ ļ░£ļŗ¼ņØś ņ¦äņĀäņØ┤ ļČĆņĪ▒ĒĢĀ Ļ▓ĮņÜ░ņŚÉļŖö ņāØĒøä 12Ļ░£ņøö ņØ┤ņĀäņŚÉ ņØĖĻ│ĄņÖĆņÜ░ņØ┤ņŗØ ņłśņłĀņØä ņŗ£Ē¢ēĒĢ£ļŗż[2]. ņØ┤ļ¤¼ĒĢ£ ņØ╝ļĀ©ņØś ņĪ░ĻĖ░ ņ▓ŁĻ░ü ņ×¼ĒÖ£ Ļ│╝ņĀĢņŚÉņä£ ņĀĢĒÖĢĒĢ£ ņ▓ŁļĀźņŚŁņ╣ś ņĖĪņĀĢņØ┤ Ļ░Ćņן ņżæņÜöĒĢ£ļŹ░, ņØ┤ļź╝ ņ£äĒĢ┤ ņ▓Łņä▒ļćīĻ░äļ░śņØæĻ▓Ćņé¼ļź╝ ņÜ░ņäĀņĀüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢ£ļŗż.
ņ▓Łņä▒ļćīĻ░äļ░śņØæņØĆ l-VĒīīņØś 5Ļ░£ņØś ņ¢æņä▒ĒīīļĪ£ ĻĄ¼ņä▒ļÉśļ®░ ĻĘĖņżæ VĒīīņØś ņŚŁņ╣śļź╝ ņ▓Łņä▒ļćīĻ░äļ░śņØæņØś ņŚŁņ╣śļĪ£ ņĀĢĒĢ£ļŗż[2]. ņ▓Łņä▒ļćīĻ░äļ░śņØæ VĒīī ņŚŁņ╣śļŖö ņŗżņĀ£ ņ▓ŁļĀźņŚŁņ╣śņÖĆ ņāüĻ┤ĆĻ┤ĆĻ│äĻ░Ć ļ¦żņÜ░ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ, ņ▓Łņä▒ļćīĻ░äļ░śņØæņØĆ Ļ░ØĻ┤ĆņĀü ņ▓ŁļĀźĻ▓Ćņé¼ļ▓Ģņ£╝ļĪ£ ļäÉļ”¼ ņØ┤ņÜ®ļÉ£ļŗż[3-5]. ņ▓Łņä▒ļćīĻ░äļ░śņØæĻ▓Ćņé¼ ņżæņŚÉ ļéśĒāĆļéśļŖö ņŚ¼ļ¤¼ ĒīīĒśĢ ņżæņŚÉņä£ VĒīīļź╝ ņ░ŠļŖö Ļ░Ćņן ņżæņÜöĒĢ£ ņ¦ĆĒæ£ļŖö ņ×Āļ│ĄĻĖ░ņØ┤ļŗż. ņĀĢņāü ņ▓ŁļĀź ņä▒ņØĖņŚÉņä£ 70-80 dBnHL Ļ░ĢļÅäņØś click ņ×ÉĻĘ╣ņØīņŚÉ ļīĆĒĢ£ VĒīī ņ×Āļ│ĄĻĖ░ļŖö 5.5-6.0 msecļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[6-8]. ĻĘĖļ¤¼ļéś Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņĀĢņāü ņ▓ŁļĀźņŚÉ ļ╣äĒĢ┤ ņ×Āļ│ĄĻĖ░Ļ░Ć ĻĖĖņ¢┤ņ¦ĆĻĖ░ ļĢīļ¼ĖņŚÉ VĒīīļź╝ ņ░ŠņØä ļĢī ņŻ╝ņØśļź╝ ņÜöĒĢ£ļŗż. Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓Ł ĒÖśņ×ÉņŚÉņä£ļŖö ņ▓ŁļĀźņØ┤ ļéśņüĀņłśļĪØ ĻĘĖļ”¼Ļ│Ā ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņĢĮĒĢ┤ņ¦łņłśļĪØ VĒīīņØś ņ×Āļ│ĄĻĖ░Ļ░Ć ļŹöņÜ▒ ĻĖĖņ¢┤ņ¦äļŗż[8]. ĒŖ╣Ē׳ ņżæņČöņ▓ŁĻ░üņĀäļŗ¼ļĪ£Ļ░Ć ļ»Ėņä▒ņłÖĒĢ£ ņśüņĢäļŖö ļÅÖņØ╝ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉņä£ ņä▒ņØĖņŚÉ ļ╣äĒĢ┤ ņ×Āļ│ĄĻĖ░Ļ░Ć ĻĖĖĻ│Ā, ņŚ░ļĀ╣ņØ┤ ņ¢┤ļ”┤ņłśļĪØ ņ×Āļ│ĄĻĖ░Ļ░Ć ļŹöņÜ▒ ĻĖĖņ¢┤ņ¦ĆĻĖ░ ļĢīļ¼ĖņŚÉ VĒīīļź╝ ņ░ŠņØä ļĢī ņ¢┤ļĀżņøĆņØ┤ ļö░ļź╝ ņłś ņ׳ļŗż[9]. ĒĢ┤ņÖĖņØś ņäĀĒ¢ēņŚ░ĻĄ¼ņŚÉņä£ ņĀĢņāü ņ▓ŁļĀźņØä Ļ░Ćņ¦ä ņśüņ£ĀņĢäņØś ņŚ░ļĀ╣Ļ│╝ ņ×ÉĻĘ╣Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ņØś ņĀĢņāüņ╣śļź╝ ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ņ£╝ļéś[6], ņĀĆņ×ÉļōżņØś ņĪ░ņé¼ Ļ▓░Ļ│╝ņŚÉ ļö░ļź┤ļ®┤ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ņśüņĢäņŚÉņä£ ņŚ░ļĀ╣, ņ▓ŁļĀźņŚŁņ╣ś, ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļŖö ļ¼ĖĒŚīņ£╝ļĪ£ ļ│┤Ļ│ĀļÉ£ ļ░öĻ░Ć ņŚåļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ļŗżņ¢æĒĢ£ ņ▓ŁļĀźņØä Ļ░Ćņ¦ä Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓Ł ņśüņĢäļź╝ ļīĆņāüņ£╝ļĪ£ ņŚ░ļĀ╣, ņ▓ŁļĀźņŚŁņ╣ś, ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢśņŚ¼ ņ▓Łņä▒ļćīĻ░äļ░śņØæĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö ņ▓ŁĻ░üņé¼ņŚÉĻ▓ī ņ£ĀņÜ®ĒĢ£ ņ░ĖĻ│Āņ×ÉļŻīļź╝ ņĀ£Ļ│ĄĒĢśĻĖ░ ņ£äĒĢ┤ ņŗ£Ē¢ēĒĢśņśĆļŗż.
ļīĆņāü ļ░Å ļ░®ļ▓Ģ
ļīĆ ņāü
2016ļģä 1ņøö 1ņØ╝ļČĆĒä░ 2021ļģä 6ņøö 1ņØ╝Ļ╣īņ¦Ć ļÅÖņĢäļīĆĒĢÖĻĄÉļ│æņøÉ ņØ┤ļ╣äņØĖĒøäĻ│╝ņŚÉņä£ ņ▓Łņä▒ļćīĻ░äļ░śņØæĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ ņāØĒøä 12Ļ░£ņøö ļ»Ėļ¦īņØś ņśüņĢä 428ļ¬ģņØś ņØśļ¼┤ĻĖ░ļĪØĻ│╝ ņ▓Łņä▒ļćīĻ░äļ░śņØæņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢśņśĆļŗż.
ņ×¼Ēā£ņŻ╝ņłś 36-40ņŻ╝ņØś ļ¦īņéŁņĢäļ¦īņØä ĒżĒĢ©ĒĢśņśĆņ£╝ļ®░, ņĀäļÅäņä▒ ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ņśüņĢäļź╝ ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ┤ Ļ│Āļ¦ē ņåīĻ▓¼ņŚÉņä£ ņżæņØ┤ ņé╝ņČ£ņĢĪņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, Ļ│Āļ¦ēņÜ┤ļÅÖņä▒Ļ│äņĖĪņāü BĒśĢņØĖ Ļ▓ĮņÜ░, ņäĀņ▓£ņä▒ ņÖĖņØ┤ļÅä ĒÅÉņćäņ”Ø, ņØ┤ņåīĻ│© ĻĖ░ĒśĢ, ĻĄ¼Ļ░£ņŚ┤ ļō▒ņØś ļæÉĻ░£ ņĢłļ®┤ĻĖ░ĒśĢņØä Ļ░Ćņ¦ä Ļ▓ĮņÜ░ļŖö ļīĆņāüņŚÉņä£ ņĀ£ņÖĖĒĢśņŚ¼ 364ļ¬ģ, 680ĻĘĆņØś ņ▓Łņä▒ļćīĻ░äļ░śņØæņØä ļČäņäØĒĢśņśĆļŗż. ņŗ£Ļ░ä Ļ░äĻ▓®ņØä ļæÉĻ│Ā ļ░śļ│Ą Ļ▓Ćņé¼ĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ņĄ£ņ┤ł Ļ▓Ćņé¼ļ¦īņØä ĒżĒĢ©ĒĢśņśĆļŗż. ņØ┤ ņżæ ņŚŁņ╣śĻ░Ć 100 dBnHLņØĖ 27ĻĘĆņÖĆ ņĄ£ļīĆņ×ÉĻĘ╣ Ļ░ĢļÅäņØĖ 100 dBnHL click ņ×ÉĻĘ╣ņØīņŚÉ ļ░śņØæņØ┤ ņŚåņŚłļŹś 114ĻĘĆļź╝ ņĀ£ņÖĖĒĢśņŚ¼, ņĄ£ņóģņĀüņ£╝ļĪ£ ņ┤Ø 318ļ¬ģ, 539ĻĘĆņØś ņ▓Łņä▒ļćīĻ░äļ░śņØæņØ┤ ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉśņŚłļŗż.
ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉ£ ņśüņĢäļōżņØĆ ņŚ░ļĀ╣Ļ│╝ ņ▓ŁļĀźņŚÉ ļö░ļØ╝ ņ¦æļŗ©ņØä ļéśļłäņ¢┤ ļČäņäØĒĢśņśĆļŗż. ņŚ░ļĀ╣ļ│äļĪ£ 0-2Ļ░£ņøö, 3-5Ļ░£ņøö, 6-8Ļ░£ņøö, 9-11Ļ░£ņøöļĪ£ ļéśļłäņŚłĻ│Ā, ņ▓ŁļĀźļ│äļĪ£ļŖö ņĀĢņāü ņ▓ŁļĀź(ņŚŁņ╣ś 20 dBnHL ņØ┤ĒĢś), Ļ▓ĮļÅä ļé£ņ▓Ł(ņŚŁņ╣ś 30-40 dBnHL), ņżæļō▒ļÅä ļé£ņ▓Ł(ņŚŁņ╣ś 50-60 dBnHL), Ļ│ĀļÅä ļé£ņ▓Ł(ņŚŁņ╣ś 70-90 dBnHL)ņ£╝ļĪ£ ļéśļłäņŚłļŗż.
ņ×ÉļŻī ņłśņ¦æ ļ░®ļ▓Ģ
ņ▓Łņä▒ļćīĻ░äļ░śņØæ Ļ▓Ćņé¼ļŖö Viking Select (Nicolet Biomedical, Madison, WI, USA) Ēś╣ņØĆ Eclipse (Interacoustics, Middelfart, Denmark) ņןļ╣äļź╝ ņé¼ņÜ®ĒĢśņŚ¼, ņśüņ£ĀņĢä ņ▓Łņä▒ļćīĻ░äļ░śņØæ Ļ▓Ćņé¼ņØś Ļ▓ĮĒŚśņØ┤ ĒÆŹļČĆĒĢ£ ņłśņäØ ņ▓ŁĻ░üņé¼Ļ░Ć ņŗ£Ē¢ēĒĢśņśĆļŗż. ļ¬©ļōĀ Ļ▓Ćņé¼ļŖö ņłśļ®┤ņ£ĀļÅäņĀ£(Pocral, chloral hydrate; Hanlim Pharm. Co., Ltd., Seoul, Korea)ļź╝ ļ│ĄņÜ®ĒĢśņŚ¼ ņłśļ®┤ ņāüĒā£ņŚÉņä£ ņŗ£Ē¢ēĒĢśņśĆļŗż. Click ņØīņØä ņ×ÉĻĘ╣ņØīņ£╝ļĪ£ ņé¼ņÜ®ĒĢśņśĆĻ│Ā Ļ▓Ćņé¼ ņŗ£ņ×æ Ļ░ĢļÅäļŖö 70 dBnHLļĪ£ ĒĢśņśĆņ£╝ļ®░ 10 dB Ļ░äĻ▓®ņ£╝ļĪ£ ņ×ÉĻĘ╣ Ļ░ĢļÅäļź╝ ņĪ░ņĀłĒĢśņśĆļŗż. ņØī ņ×ÉĻĘ╣ Ēøä 5-10 ms ņé¼ņØ┤ņŚÉ ļéśĒāĆļéśļŖö ņ¢æņä▒ĒīīļĪ£ņä£ 2ĒÜī ļ░śļ│Ą ņĖĪņĀĢņŚÉņä£ ĒīīĒśĢņØś ņ×¼Ēśäņä▒ņØ┤ ņ׳Ļ│Ā, ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņżäņ¢┤ļō”ņŚÉ ļö░ļØ╝ ņ×Āļ│ĄĻĖ░Ļ░Ć ņĀÉņ¦äņĀüņ£╝ļĪ£ ņŚ░ņןļÉśĻ│Ā ņ¦äĒÅŁņØ┤ ņĀÉņ¦äņĀüņ£╝ļĪ£ ņ×æņĢäņ¦ĆļŖö Ļ▓ĮņÜ░ņŚÉ VĒīīļĪ£ ĒīÉņĀĢĒĢśņśĆļŗż.
Ļ░ü ņĢäļÅÖļ│ä VĒīī ņŚŁņ╣śņÖĆ ļ¬©ļōĀ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļīĆĒĢ£ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢśņśĆļŗż.
ļČäņäØ ļ░®ļ▓Ģ
ņøöļĀ╣ņ£╝ļĪ£ Ļ│äņé░ļÉ£ ņŚ░ļĀ╣, ņ▓ŁļĀźņŚŁņ╣ś, ĻĘĖļ”¼Ļ│Ā ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ļČäņäØĒĢśņśĆļŗż. ĒåĄĻ│ä ļČäņäØņØĆ SPSS (version 26.0; IBM Corp., Armonk, NY, USA) ĒåĄĻ│ä ĒöäļĪ£ĻĘĖļשņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņäĀĒśĢĒś╝ĒĢ®ļ¬©ļŹĖ(linear mixed model, LMM) ļ░®ļ▓ĢņØä ņĀüņÜ®ĒĢśņŚ¼ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, p Ļ░ÆņØ┤ 0.05ļ│┤ļŗż ņ×æņ£╝ļ®┤ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢ£ Ļ▓āņ£╝ļĪ£ Ļ░äņŻ╝ĒĢśņśĆļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ļÅÖņĢäļīĆĒĢÖĻĄÉļ│æņøÉ ņ×äņāüņŗ£ĒŚśņ£żļ”¼ņ£äņøÉĒÜīņØś ņŗ¼ņØśļź╝ Ļ▒░ņ│É ņŖ╣ņØĖņØä ļ░øņØĆ Ēøä ņŗ£Ē¢ēĒĢśņśĆļŗż(ņŖ╣ņØĖļ▓łĒśĖ: DAUHIRB 22-135).
Ļ▓░ Ļ│╝
ļīĆņāüņ×ÉņØś ņŚ░ļĀ╣ ļČäĒżņÖĆ Ļ░ü ņŚ░ļĀ╣ņ¦æļŗ©ļ│ä ņ▓ŁļĀź ļČäĒż
ļé©ņĢäĻ░Ć 182ļ¬ģ, ņŚ¼ņĢäĻ░Ć 136ļ¬ģņØ┤ņŚłĻ│Ā, ņŚ░ļĀ╣ ļČäĒżļŖö 0-2Ļ░£ņøö 107ļ¬ģ, 3-5Ļ░£ņøö 81ļ¬ģ, 6-8Ļ░£ņøö 70ļ¬ģ, 9-11Ļ░£ņøö 60ļ¬ģņØ┤ņŚłļŗż. ņ▓ŁļĀźņŚŁņ╣śļŖö ņĀĢņāüņØ┤ 59.4% (320ĻĘĆ), Ļ▓ĮļÅä ļé£ņ▓ŁņØ┤ 15.6% (84ĻĘĆ), ņżæļō▒ļÅä ļé£ņ▓ŁņØ┤ 15.9% (86ĻĘĆ), Ļ│ĀļÅä ļé£ņ▓ŁņØ┤ 9.1% (49ĻĘĆ)ņśĆļŗż(Table 1).
ņ▓ŁļĀźĻ│╝ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ņØś ļ│ĆĒÖö
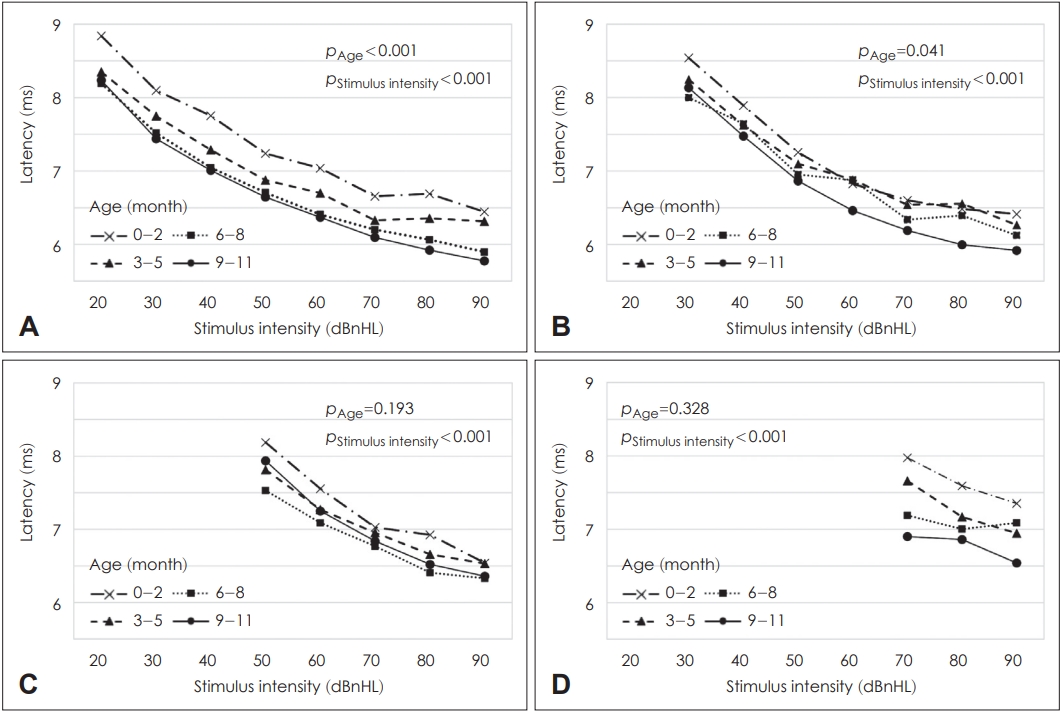
ļ│Ė ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉ£ ņśüņĢäļź╝ ņ▓ŁļĀźņŚÉ ļö░ļØ╝ ļäż ņ¦æļŗ©ņ£╝ļĪ£ ļéśļłäņ¢┤ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ļČäņäØĒĢśņśĆļŗż(Fig. 1). ļäż ņ¦æļŗ© ļ¬©ļæÉņŚÉņä£ ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņ╗żņ¦łņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(p’╝£0.001, LMM). ļśÉĒĢ£ ņ▓ŁļĀźņŚŁņ╣śĻ░Ć ļåÆņØäņłśļĪØ ļÅÖņØ╝ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉņä£ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī ņŚ░ņןļÉśņ¢┤ ņ׳ņŚłļŗż(p’╝£0.001, LMM).
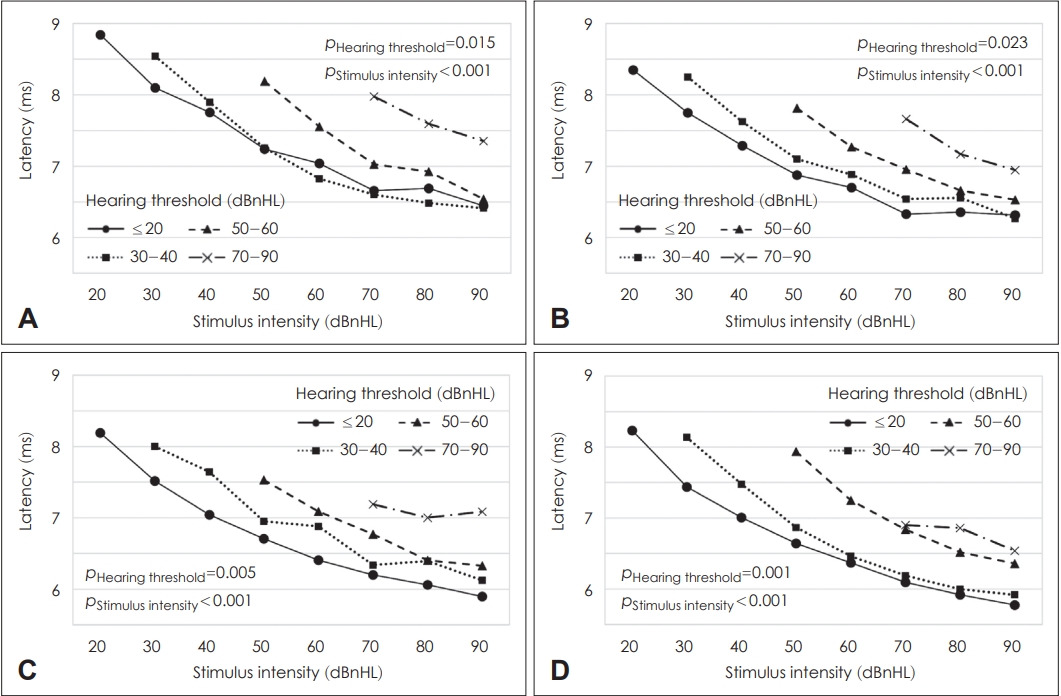
ņŚ░ļĀ╣ņŚÉ ļö░ļźĖ ņ×Āļ│ĄĻĖ░ ļČäņäØņŚÉņä£ļÅä, ļ¬©ļōĀ ņŚ░ļĀ╣ņ¦æļŗ©ņŚÉņä£ ņ▓ŁļĀź ņŚŁņ╣śĻ░Ć ļåÆņØäņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī ņ”ØĻ░ĆĒĢśņśĆĻ│Ā(p=0.015 for 0-2 months-old infants, p=0.023 for 3-5 months-old infants, p=0.005 for 6-8 months-old infants, p=0.001 for 9-11 months-old infants, LMM), ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņ”ØĻ░ĆĒĢĀņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(p’╝£0.001 for all age subgroups, LMM) (Fig. 2).
ņŚ░ļĀ╣Ļ│╝ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ņØś ļ│ĆĒÖö
ļ│Ė ņŚ░ĻĄ¼ņŚÉ ĒżĒĢ©ļÉ£ ņśüņĢäļź╝ Ļ▓Ćņé¼ ņŗ£ ņŚ░ļĀ╣ņŚÉ ļö░ļØ╝ ļäż ņ¦æļŗ©ņ£╝ļĪ£ ļéśļłäņ¢┤ ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ļČäņäØĒĢśņśĆļŗż(Fig. 3 and Table 2). ņĀĢņāü ņ▓ŁļĀź ļ░Å Ļ▓ĮļÅä ļé£ņ▓Ł ņ¦æļŗ©ņŚÉņä£ļŖö ņŚ░ļĀ╣ņØ┤ ņ”Ø Ļ░ĆĒĢĀņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(p’╝£0.001 for normal hearing infants, p=0.041 for mild hearing loss infants, LMM). ņżæļō▒ļÅä ļé£ņ▓Ł ļ░Å Ļ│ĀļÅä ļé£ņ▓Ł ņ¦æļŗ©ņŚÉņä£ļŖö ņŚ░ļĀ╣ņØ┤ ņ”ØĻ░ĆĒĢĀņłśļĪØ ņ×Āļ│ĄĻĖ░ļŖö Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆņ£╝ļéś ĒåĄĻ│äņĀü ņ£ĀņØśņä▒ņØĆ ņŚåņŚłļŗż(p=0.193 for moderate hearing loss infants, p=0.328 for severe to profound hearing loss infants, LMM). ļäż ņ▓ŁļĀź ņ¦æļŗ© ļ¬©ļæÉņŚÉņä£ ņĀä ņŚ░ļĀ╣ņŚÉ Ļ▒Ėņ│É ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņ”ØĻ░ĆĒĢĀņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśņśĆļŗż(p’╝£0.001 for all hearing subgroups, LMM).
ņŚ░ļĀ╣Ļ│╝ ņ▓ŁļĀźņŚÉ ļö░ļźĖ 70 dBnHL click ņ×ÉĻĘ╣ņØīņŚÉ ļīĆĒĢ£ VĒīī ņ×Āļ│ĄĻĖ░
ņ▓Łņä▒ļćīĻ░äļ░śņØæĻ▓Ćņé¼ņØś ņŗ£ņ×æ Ļ░ĢļÅäņØĖ 70 dBnHL ņ×ÉĻĘ╣ņØīņŚÉ ļīĆĒĢ£ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ļČäņäØĒĢśņśĆļŗż(Fig. 4). 70 dBnHL ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉņä£ VĒīī ĒÅēĻĘĀ ņ×Āļ│ĄĻĖ░ļŖö ņĀĢņāü ņ▓ŁļĀźĻĄ░ņŚÉņä£ 6.36 msec, Ļ▓ĮļÅä ļé£ņ▓ŁĻĄ░ņŚÉņä£ 6.43 msec, ņżæļō▒ļÅä ļé£ņ▓ŁĻĄ░ņŚÉņä£ 6.91 msec, Ļ│ĀļÅä ļé£ņ▓ŁĻĄ░ņŚÉņä£ 7.62 msecņśĆņ£╝ļ®░, ņŚ░ļĀ╣ņØ┤ ņ”ØĻ░ĆĒĢ©ņŚÉ ļö░ļØ╝ ņ×Āļ│ĄĻĖ░Ļ░Ć Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż.
Ļ│Ā ņ░░
ņ▓Łņä▒ļćīĻ░äļ░śņØæņØĆ ņåīļ”¼ņ×ÉĻĘ╣ņŚÉ ņØśĒĢ┤ ņ▓ŁņŗĀĻ▓ĮņŚÉņä£ ļćīĻ░äņŚÉ ņØ┤ļź┤ļŖö ņ▓ŁĻ░üņĀäļŗ¼ļĪ£ņŚÉņä£ ļ░£ņāØĒĢśļŖö ĒÖ£ļÅÖņĀäņ£äļź╝ ĻĖ░ļĪØĒĢ£ Ļ▓āņ£╝ļĪ£ 5Ļ░£ņØś ņ¢æņä▒ĒīīļĪ£ ĻĄ¼ņä▒ļÉ£ļŗż. ņ▓Łņä▒ļćīĻ░äļ░śņØæņØś IĒīīļŖö ņ▓ŁņŗĀĻ▓Į, IIĒīīļŖö ņÖĆņÜ░ĒĢĄ, IIIĒīīļŖö ņāüņś¼ļ”¼ļĖīļ│ĄĒĢ®ņ▓┤, IVĒīīļŖö ņÖĖņĖĪ ņä¼ņ£ĀļīĆ, VĒīīļŖö ĒĢśĻĄ¼ņŚÉņä£ ĻĖ░ņøÉĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[10-12]. VĒīīĻ░Ć ļéśĒāĆļéśļŖö ņĄ£ņåī ņ×ÉĻĘ╣ Ļ░ĢļÅäļź╝ ņ▓Łņä▒ļćīĻ░äļ░śņØæņØś ņŚŁņ╣śļĪ£ ņĀĢĒĢśļ®░ VĒīī ņŚŁņ╣śļź╝ ĒīÉņĀĢĒĢśļŖö Ļ░Ćņן ņżæņÜöĒĢ£ ņ¦ĆĒæ£ ņżæ ĒĢśļéśļŖö ņ×Āļ│ĄĻĖ░ņØ┤ļŗż.
VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņČ£ņāØ Ēøä ņĀÉņ¦äņĀüņ£╝ļĪ£ Ļ░ÉņåīĒĢ£ļŗż. ņ▓ŁņŗĀĻ▓ĮņŚÉņä£ ĒĢśĻĄ¼ņŚÉ ņØ┤ļź┤ļŖö ļćīĻ░äņØś ņ▓ŁĻ░üņĀäļŗ¼ļĪ£ņŚÉņä£ Ēā£ņĢä 26-29ņŻ╝ ņé¼ņØ┤ņŚÉ ņČĢņéŁņØś ņłśņ┤łĒÖöĻ░Ć ļ░£ņāØĒĢśĻ│Ā, ņāØĒøä 1ļģäĻ╣īņ¦Ć ņłśņ┤łĒÖö ļ░ĆļÅäĻ░Ć ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢ£ļŗż[13]. ļćīĻ░äņØä ĒåĄĒĢ£ ņ▓ŁĻ░üņĀäļŗ¼ļĪ£ņØś ņłśņ┤łĒÖö ņ”ØĻ░ĆļĪ£ ņØĖĒĢ┤ ņŗĀĻ▓ĮņĀäļÅäņåŹļÅäĻ░Ć ļ╣©ļØ╝ņĀĖ VĒīīņØś ņ×Āļ│ĄĻĖ░Ļ░Ć Ļ░ÉņåīĒĢ£ļŗż[9]. VĒīī ņ×Āļ│ĄĻĖ░ļŖö ņāØĒøä 2ņäĖĻ▓ĮĻ╣īņ¦Ć ņĀÉņ¦äņĀüņ£╝ļĪ£ Ļ░ÉņåīĒĢśņŚ¼ ņä▒ņØĖņØś ņłśņżĆņŚÉ ļÅäļŗ¼ĒĢśļ®░, ņØ┤Ēøä ņØ╝ņĀĢĒĢśĻ▓ī ņ£Āņ¦ĆļÉśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[9,13,14].
Gorga ļō▒[6]ņØĆ ņĀĢņāü ņ▓ŁļĀź(20 dBnHL ņ×ÉĻĘ╣ņØīņŚÉ VĒīīĻ░Ć ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░)ņØä Ļ░Ćņ¦ä 36Ļ░£ņøö ņØ┤ĒĢś ņśüņ£ĀņĢä 535ļ¬ģņØś VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢśņśĆļŗż. ņØ┤ ņżæ 238ļ¬ģņØ┤ 12Ļ░£ņøö ņØ┤ĒĢś ņśüņĢäņśĆļŖöļŹ░, 80 dBnHL click ņ×ÉĻĘ╣ņØīņŚÉ ļīĆĒĢ£ VĒīī ĒÅēĻĘĀ ņ×Āļ│ĄĻĖ░ļŖö 3-6Ļ░£ņøöņŚÉ 6.253 msec, 6-9Ļ░£ņøöņŚÉ 6.101 msec, 9-12Ļ░£ņøöņŚÉ 5.899 msecļĪ£, ņČ£ņāØ Ēøä VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ņĀÉņ¦äņĀüņ£╝ļĪ£ ņżäņ¢┤ļō£ļŖö ņ¢æņāüņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. ņŚ░ĻĄ¼ņŚÉņä£ ņé¼ņÜ®ĒĢ£ ņĄ£ņåī ņ×ÉĻĘ╣ Ļ░ĢļÅäņØĖ 20 dBnHL ņ×ÉĻĘ╣ņØīņŚÉ ļīĆĒĢ£ VĒīī ĒÅēĻĘĀ ņ×Āļ│ĄĻĖ░ļŖö 3-6Ļ░£ņøöņŚÉ 8.717 msec, 6-9Ļ░£ņøöņŚÉ 8.591 msec, 9-12Ļ░£ņøöņŚÉ 8.310 msecļĪ£ ņĄ£ņåī ņ×ÉĻĘ╣ Ļ░ĢļÅäņŚÉņä£ļÅä ņŚ░ļĀ╣ņØ┤ ņ”ØĻ░ĆĒĢ©ņŚÉ ļö░ļØ╝ VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć Ļ░ÉņåīĒĢśņśĆļŗż.
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĀĢņāü ņ▓ŁļĀźņØä Ļ░Ćņ¦ä ņśüņĢäņÖĆ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ņśüņĢäļź╝ ļ¬©ļæÉ ĒżĒĢ©ĒĢśņŚ¼ ņŚ░ļĀ╣, ņ×ÉĻĘ╣ Ļ░ĢļÅä, ĻĘĖļ”¼Ļ│Ā ļé£ņ▓ŁņØś ņĀĢļÅäņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢśņśĆļŗż. ņŚ░ļĀ╣ņØ┤ ņ”ØĻ░ĆĒĢĀņłśļĪØ, ĻĘĖļ”¼Ļ│Ā ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć ņ╗żņ¦łņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ņ£ĀņØśĒĢśĻ▓ī Ļ░ÉņåīĒĢśĻ│Ā, ļé£ņ▓ŁņØ┤ ņŗ¼ĒĢĀņłśļĪØ VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ņ£ĀņØśĒĢśĻ▓ī ļŖśņ¢┤ļéśļŖö Ļ▓āņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż. ļśÉĒĢ£ ņĀĢņāü ņ▓ŁļĀźĻĄ░ņŚÉņä£ļŖö ņāØĒøä 6Ļ░£ņøöĻ╣īņ¦Ć VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ļ╣Āļź┤Ļ▓ī Ļ░ÉņåīĒĢśļŗżĻ░Ć ņāØĒøä 12Ļ░£ņøöĻ╣īņ¦Ć ņÖäļ¦īĒĢśĻ▓ī Ļ░ÉņåīĒĢ£ļŹ░ ļ╣äĒĢ┤ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁĻĄ░ņŚÉņä£ļŖö ņāØĒøä 12Ļ░£ņøöĻ╣īņ¦Ć VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ļ╣äĻĄÉņĀü ņØ╝ņĀĢĒĢśĻ▓ī Ļ░ÉņåīĒĢśļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņśĆļŗż(Fig. 3). ņØ┤ļŖö ņĀĢņāü ņ▓ŁļĀź ņśüņĢäņÖĆ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓Ł ņśüņĢäņØś ļćīĻ░äņØä ĒåĄĒĢ£ ņżæņČöņ▓ŁĻ░üļĪ£ņØś ļ░£ļŗ¼ ņ¢æņāüņØ┤ ņāüņØ┤ĒĢĀ ņłś ņ׳ņØīņØä ņŗ£ņé¼ĒĢśļŖö ņåīĻ▓¼ņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż.
ņ×ÉĻĘ╣ Ļ░ĢļÅäĻ░Ć Ļ░ÉņåīĒĢśļ®┤ VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ĻĖĖņ¢┤ņ¦ĆļŖöļŹ░, Ļ░Ģņ×ÉĻĘ╣ņŚÉņä£ļŖö ņ×ÉĻĘ╣ Ļ░ĢļÅä Ļ░ÉņåīņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ ņŚ░ņןņØś ņĀĢļÅäĻ░Ć ņĀüņØĆ ļ░śļ®┤, ņĢĮņ×ÉĻĘ╣ņŚÉņä£ļŖö ņ×ÉĻĘ╣ Ļ░ĢļÅä Ļ░ÉņåīņŚÉ ļö░ļźĖ VĒīī ņ×Āļ│ĄĻĖ░ ņŚ░ņןņØ┤ ļæÉļō£ļ¤¼ņ¦äļŗż. ņäĀĒ¢ē ņŚ░ĻĄ¼ņŚÉņä£ 60 dBnHL ņØ┤ņāü Ļ░ĢļÅäņŚÉņä£ļŖö 10 dB ļ¦łļŗż ņĢĮ 0.1-0.2 msec, 60 dBnHL ņØ┤ĒĢś Ļ░ĢļÅäņŚÉņä£ļŖö 10 dB ļ¦łļŗż ņĢĮ 0.5-0.6 msecņØś VĒīī ņ×Āļ│ĄĻĖ░ ļ│ĆĒÖöĻ░Ć ļ░£ņāØĒĢ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳ļŗż[15]. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņ×ÉĻĘ╣ Ļ░ĢļÅäņØś Ļ░ÉņåīņŚÉ ļö░ļØ╝ VĒīī ņ×Āļ│ĄĻĖ░Ļ░Ć ņ”ØĻ░ĆĒĢśņśĆĻ│Ā, ņĀĢņāü ņ▓ŁļĀźĻĄ░Ļ│╝ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁĻĄ░ ļ¬©ļæÉņŚÉņä£ Ļ░Ģņ×ÉĻĘ╣ņŚÉ ļ╣äĒĢ┤ ņĢĮņ×ÉĻĘ╣ņŚÉņä£ ņ×Āļ│ĄĻĖ░ Ļ░ÉņåīĒÅŁņØ┤ ņ╗żņ¦ĆļŖö Ļ▓ĮĒ¢źņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(Fig. 1).
Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņĀĢņāü ņ▓ŁļĀź Ēś╣ņØĆ Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓ŁņØä Ļ░Ćņ¦ä 12Ļ░£ņøö ļ»Ėļ¦ī ņśüņĢä 318ļ¬ģņØś 539ĻĘĆļź╝ ļīĆņāüņ£╝ļĪ£ ņŚ░ļĀ╣(0-11Ļ░£ņøö), ņ▓ŁļĀź ņŚŁņ╣ś(ņĀĢņāü-Ļ│ĀļÅä Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ļé£ņ▓Ł), ĻĘĖļ”¼Ļ│Ā ņ×ÉĻĘ╣ Ļ░ĢļÅä(20-90 dBnHL)ņŚÉ ļö░ļźĖ ņ▓Łņä▒ļćīĻ░äļ░śņØæ VĒīī ņ×Āļ│ĄĻĖ░ļź╝ ņĪ░ņé¼ĒĢśņŚ¼ ĻĘĖ ĒÅēĻĘĀņ╣śļź╝ Ēæ£ņżĆņśżņ░©ņÖĆ ĒĢ©Ļ╗ś ņĀ£ņŗ£ĒĢśņśĆļŗż. ļ│Ė ņŚ░ĻĄ¼ņØś Ļ▓░Ļ│╝ņ╣śļŖö ņśüņĢäņØś ņ▓Łņä▒ļćīĻ░äļ░śņØæ Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö ņ▓ŁĻ░üņé¼ņŚÉĻ▓ī ņ£ĀņÜ®ĒĢ£ ņ░ĖĻ│Āņ×ÉļŻīĻ░Ć ļÉĀ Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉ£ļŗż.