м„ң лЎ
м–‘мӘҪ к·Җмқҳ мһ‘мқҖ мІӯл Ҙм—ӯм№ҳ м°ЁмқҙлҸ„ лӢӨмһҗк°„мқҳ лҢҖнҷ”к°Җ л§ҺмқҖ мҶҢмқҢ нҷҳкІҪм—җм„ңлҠ” л¬ёмһҘмқҳ мқём§Җм—җ м ңн•ңмқ„ мЈјл©°[1], н•ңмӘҪ к·Җмқҳ м „лҶҚ мӢң лі‘ліҖ мӘҪм—җм„ң л°ңмғқн•ҳлҠ” мҶҢлҰ¬лҘј л“Јм§Җ лӘ»н• лҝҗ м•„лӢҲлқј, мҶҢмқҢ н•ҳм—җм„ң м–ҙмқҢмқҙн•ҙлҸ„ л°Ҹ мҶҢлҰ¬мқҳ л°©н–Ҙ нғҗм§Җм—җ м–ҙл ӨмӣҖмқ„ кІӘлҠ”лӢӨ[2]. мқҙлҘј к·№ліөн•ҳкё° мң„н•ҙ мҶҗмғҒлҗң к·Җмқҳ мІӯл Ҙмқ„ нҳём „мӢңнӮӨлҠ” мқёкіөмҷҖмҡ°мҲҳмҲ , м „лҶҚмқҙ мһҲлҠ” к·ҖлЎң л“Өм–ҙмҳӨлҠ” мҶҢлҰ¬лҘј л°ҳлҢҖмӘҪ к·ҖлЎң м „лӢ¬н•ҳлҠ” нҒ¬лЎңмҠӨ ліҙмІӯкё°(contralateral routing of signal [CROS] hearing aid)мҷҖ мқҙмӢқнҳ• кіЁм „лҸ„ ліҙмІӯкё°(bone conduction implant)лҘј мғқк°Ғн•ҙ ліј мҲҳ мһҲлӢӨ. мқҙ мӨ‘ кіЁм „лҸ„ ліҙмІӯкё°лҠ” мҳӨлһҳ м „л¶Җн„° мІӯл Ҙмһ¬нҷңм—җ мқҙмҡ©лҗҳм–ҙ мҷ”кі м„ мІңм„ұ мҷёмқҙкё°нҳ•, л§Ңм„ұ нҷ”лҶҚм„ұ мӨ‘мқҙм—ј, мқјмёЎм„ұ кі лҸ„лӮңмІӯмқҙ мһҲлҠ” нҷҳмһҗлӮҳ кі мӢқм Ғмқё ліҙмІӯкё° мӮ¬мҡ©м—җ мӢӨнҢЁн•ң нҷҳмһҗм—җкІҢ мӮ¬мҡ©мқ„ кі л Өн• мҲҳ мһҲлӢӨ[3].
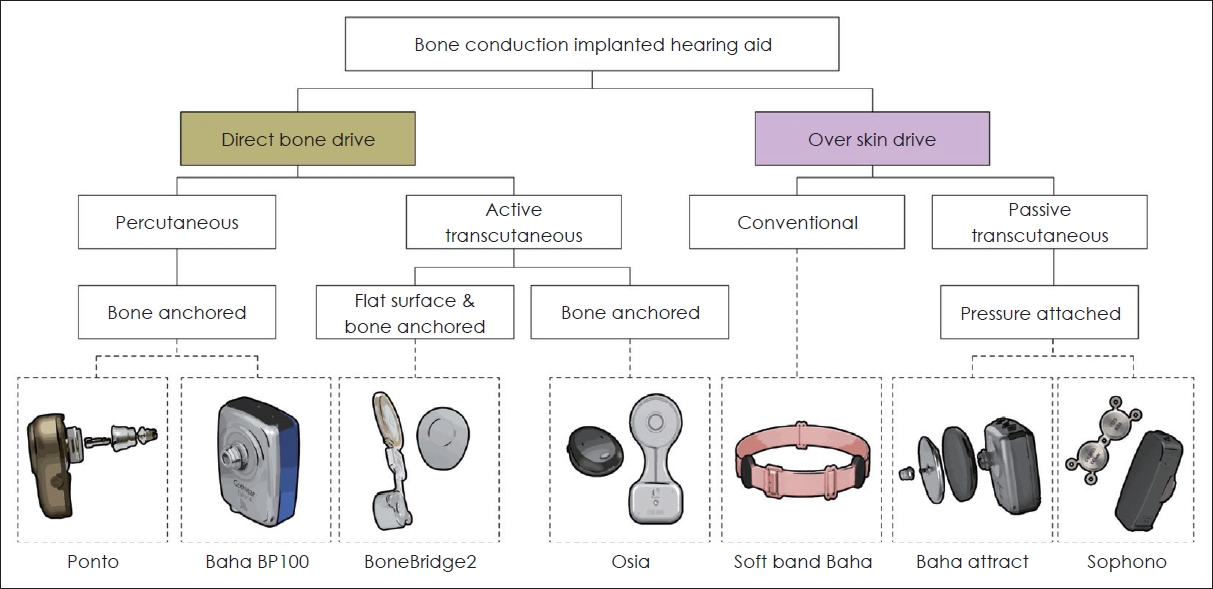
Osiaв“Ү2 system (Cochlear, Sydney, Australia)мқҖ мҷёл¶Җ н”„лЎңм„ём„ңмҷҖ мһ„н”ҢлһҖнҠё мӮ¬мқҙм—җ кІҪн”јм ҒмңјлЎң м—°кІ°лҗҳл©° м••м „мһҗк·№(piezoelectric)л°©мӢқмқ„ мқҙмҡ©н•ҳлҠ” мғҲлЎңмҡҙ лҠҘлҸҷн”јн•ҳл°©мӢқ4-8)мқҳ кіЁм „лҸ„ ліҙмІӯкё°мқҙлӢӨ(Fig. 1). Osiaв“Ү2лҠ” лҜёкөӯм—җм„ң 2019л…„ 11мӣ” 15мқјм—җ Food and Drug Administration (FDA) мҠ№мқёмқ„ л°ӣм•ҳкі 12к°ңмӣ”к°„мқҳ large cohortк°Җ мӢңн–үлҗҳм—Ҳмңјл©°[9] Lau л“ұ[4]м—җ мқҳн•ҙ Osiaв“Ү2мқҳ м•Ҳм „м„ұкіј мң нҡЁм„ұмқҙ мһ…мҰқлҗҳм—ҲмңјлӮҳ, көӯлӮҙ л¬ён—ҢмғҒ Osiaв“Ү2лҘј нҶөн•ң мІӯк°Ғмһ¬нҷңмқҖ ліҙкі лҗң л°”к°Җ м—ҶлӢӨ. мқҙм—җ м Җмһҗл“ӨмқҖ мҲҳмҲ нӣ„ л°ңмғқн•ң мқјмёЎм„ұ кі лҸ„ лӮңмІӯ нҷҳмһҗм—җм„ң Osiaв“Ү2 мқҙмӢқмқ„ нҶөн•ҙ мІӯл Ҙмһ¬нҷңмқ„ мӢңн–үн•ң 2мҳҲлҘј кІҪн—ҳн•ҳм—¬ мқҙлҘј л¬ён—Ң кі м°°кіј н•Ёк»ҳ ліҙкі н•ҳкі мһҗ н•ңлӢӨ.
мҰқ лЎҖ
мҰқлЎҖ 1
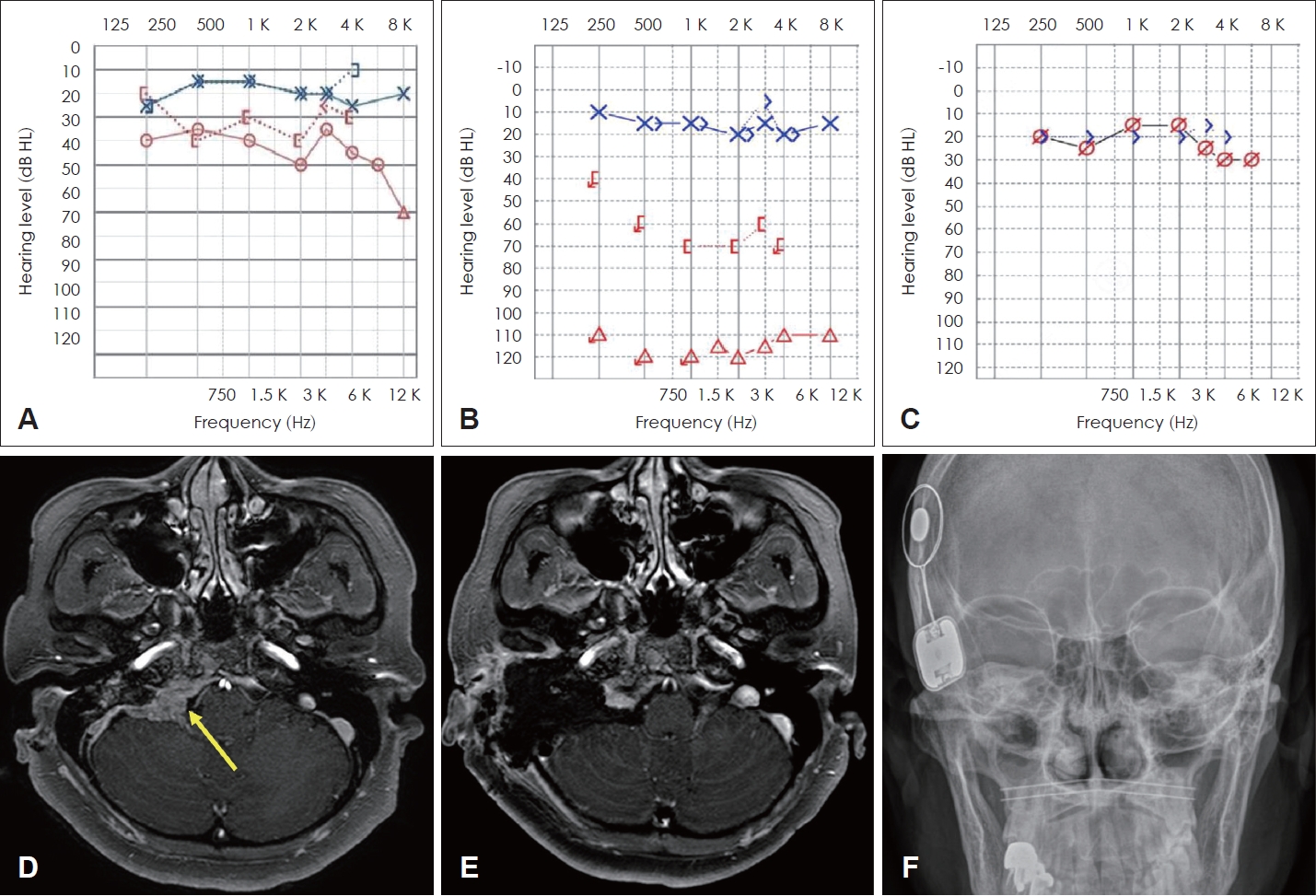
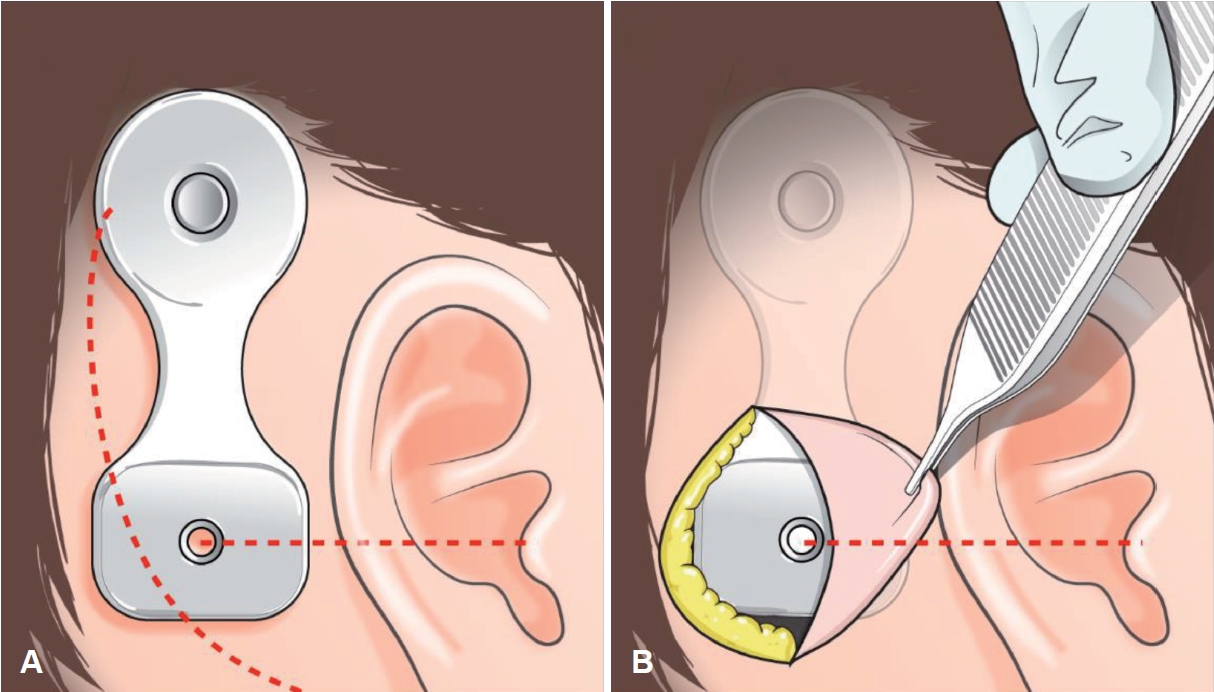
мҡ°мёЎ кІҪм •л§Ҙкө¬ мӮ¬кө¬мў…(Fig. 2D)мңјлЎң 2016л…„ fallopian bridge мҲ мӢқмқ„ мқҙмҡ©н•ҳм—¬ м Ҳм ңмҲ мқ„ мӢңн–ү л°ӣмқҖ 60м„ё м—¬мһҗ нҷҳмһҗк°Җ мҲҳмҲ м „ нҷҳмёЎмқҳ кІҪлҸ„ м „лҸ„м„ұ лӮңмІӯ мҶҢкІ¬мқ„ ліҙмҳҖмңјлӮҳ мҲҳмҲ нӣ„ мӢ¬лҸ„ лӮңмІӯмңјлЎң мёЎм •лҗҳм—ҲлӢӨ(Fig. 2A and B). мҲҳмҲ нӣ„ 5л…„к°„ мӢңн–үн•ң 추м Ғ кҙҖм°°мғҒ мһ¬л°ң мҶҢкІ¬мқҖ кҙҖм°°лҗҳм§Җ м•Ҡм•ҳкі (Fig. 2E), нҳём „лҗҳм§Җ м•ҠлҠ” нҷҳмһҗмқҳ мҡ°мёЎ лӮңмІӯм—җ лҢҖн•ң мһ¬нҷңмқ„ кі„нҡҚн•ҳмҳҖлӢӨ. мқҙм „ мҲҳмҲ мӢң ліҖнҳ•лҗң н•ҙл¶Җн•ҷм Ғ кө¬мЎ° л°Ҹ мҷҖмҡ°мқҳ кіЁнҷ” мҶҢкІ¬мқҙ мһҲкё°м—җ мқёкіөмҷҖмҡ°лҠ” м Ғн•©н•ҳм§Җ м•Ҡм•„ кіЁм „лҸ„ мһ„н”ҢлһҖнҠё мқҙмӢқмқҙ н•©лӢ№н•ҳлӢӨкі нҢҗлӢЁн•ҳмҳҖлӢӨ. мҲҳмҲ мқҖ көӯмҶҢл§Ҳм·Ён•ҳм—җ мӢңн–үлҗҳм—ҲлӢӨ. мӢӨлҰ¬мҪҳ нҳ•нҢҗ(template)мқ„ нҶөн•ҙ м Ҳк°ң л¶Җ분мқ„ н‘ңмӢңн•ҳмҳҖлӢӨ. мқҙм „ мҲҳмҲ мӢң м Ҳк°ңм„ мқ„ мқҙмҡ©н•ҳмҳҖмңјл©° лјҲлҘј л…ём¶ңмӢңнӮЁ нӣ„ BI300 implant fixture (Cochlear, Sydney, Australia)мқҳ м •нҷ•н•ң мң„м№ҳлҘј н‘ңмӢңн•ң л’Ө, burrлҘј мқҙмҡ©н•ҳм—¬ drillingмқ„ мӢңн–үн•ҳмҳҖлӢӨ. мқҙнӣ„ BI300 implant fixureлҘј кі м •лӮҳмӮ¬лЎң BI300 implantм—җ м—°кІ°н•ҳкі м Ҳк°ңл¶Җмң„ лҙүн•©мқ„ мӢңн–үн•ҳмҳҖлӢӨ(Figs. 2F and 3). Osiaв“Ү2 мқҙмӢқ 1к°ңмӣ” нӣ„ мҲңмқҢмІӯл ҘкІҖмӮ¬мғҒ мҡ°мёЎ мІӯл Ҙм—ӯм№ҳ 25 dB HL, 5к°ңмӣ” нӣ„ мҲңмқҢмІӯл ҘкІҖмӮ¬мғҒ мҡ°мёЎ мІӯл Ҙм—ӯм№ҳ 21 dB HLлЎң нҳём „лҗҳм—ҲлӢӨ(Fig. 2C). Korean Hearing in Noise Test (K-HINT)мғҒ мҲҳмҲ м „ Reception Threshold for Speech (RTS)лҠ” 30.0 dB, мқҙнӣ„ 26.6 dBлЎң н–ҘмғҒлҗҳм—Ҳмңјл©° ліөн•©мһЎмқҢмЎ°кұҙм—җм„ң нҸүк· signal to noise ratio (SNR)мқҖ Osiaв“Ү2 м°©мҡ© мӢң 1.8 SNRм—җм„ң 0.0 SNRлЎң к°җмҶҢн•ҳмҳҖлӢӨ. Osiaв“Ү2 мқҙмӢқ мқҙнӣ„ мҷёлһҳм—җм„ң 6к°ңмӣ”м§ё 추м Ғ кҙҖм°° мӨ‘мқҙл©°, мғҒмІҳ л°Ҹ н”јл¶Җ н•©лі‘мҰқ м—Ҷмқҙ к°ңм„ лҗң мІӯл ҘмңјлЎң нҷҳмһҗлҠ” мҲҳмҲ кІ°кіјм—җ л§Өмҡ° л§ҢмЎұн•ҳмҳҖлӢӨ.
мҰқлЎҖ 2
73м„ё м—¬мһҗ нҷҳмһҗк°Җ ліёмӣҗ мқҙ비мқёнӣ„кіјм—җм„ң м–‘мёЎ мӨ‘мқҙм—јмңјлЎң 2012л…„кіј 2013л…„мңјлЎң лӮҳлҲ„м–ҙ м–‘мёЎ мң м–‘лҸҷ м Ҳм ңмҲ л°Ҹ кі мӢӨм„ұнҳ•мҲ мқ„ мӢңн–ү л°ӣм•ҳлӢӨ(Fig. 4D). мўҢмёЎ мҲҳмҲ мӨ‘ л°ңмғқн•ң мқҳмқём„ұ мҶҗмғҒм—җ мқҳн•ҙ мўҢмёЎмқҳ мӢ¬лҸ„ лӮңмІӯмқҙ л°ңмғқн–Ҳмңјл©° мҡ°мёЎмқҖ мӨ‘л“ұлҸ„ нҳјн•©м„ұ лӮңмІӯмқҙ кі„мҶҚ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 4A and B). мҲҳмҲ нӣ„ 8л…„ лҸҷм•Ҳ мһ¬л°ң мҶҢкІ¬мқҙ м—Ҷм—Ҳкё°м—җ нҳём „лҗҳм§Җ м•ҠлҠ” нҷҳмһҗмқҳ мўҢмёЎ лӮңмІӯм—җ лҢҖн•ҙ мһ¬нҷңмқ„ кі„нҡҚн•ҳмҳҖлӢӨ. мқҳмқём„ұ лҜёлЎң мҶҗмғҒмңјлЎң мқён•ң мҷҖмҡ°кіЁнҷ” мҶҢкІ¬мқҙ нҷ•мқёлҗҳм—Ҳкё°м—җ(Fig. 4E) кіЁм „лҸ„ мһ„н”ҢлһҖнҠё мҲҳмҲ мқҙ н•©лӢ№н•ҳлӢӨкі нҢҗлӢЁн•ҳмҳҖлӢӨ. көӯмҶҢл§Ҳм·Ён•ҳм—җ лҸҷмқјн•ң л°©лІ•мңјлЎң мҲҳмҲ мқ„ 진н–үн•ҳмҳҖмңјл©°(Fig. 4F), Osiaв“Ү2 мқҙмӢқ 2к°ңмӣ” нӣ„ мҲңмқҢмІӯл ҘкІҖмӮ¬мғҒ мўҢмёЎ мІӯл Ҙм—ӯм№ҳ 39 dB HL, 7к°ңмӣ” нӣ„ мҲңмқҢмІӯл ҘкІҖмӮ¬мғҒ мҡ°мёЎ мІӯл Ҙм—ӯм№ҳ 41 dB HLлЎң нҳём „лҗҳм—ҲлӢӨ(Fig. 4C). K-HINTмғҒ мҲҳмҲ м „ RTSлҠ” 76.9 dB, мқҙнӣ„ 43.36 dBлЎң н–ҘмғҒлҗҳм—Ҳмңјл©°, нҸүк· SNRмқҖ 12.9 SNRм—җм„ң мҲ нӣ„ 0.8 SNRлЎң нҳ„м Җн•ҳкІҢ к°җмҶҢн•ҳмҳҖлӢӨ. мҲ нӣ„ 7к°ңмӣ” лҸҷм•Ҳ н•©лі‘мҰқ м—Ҷмқҙ 추м ҒкҙҖм°° мӨ‘мқҙл©° нҷҳмһҗмқҳ л§ҢмЎұлҸ„лҠ” лҶ’мқҖ мғҒнғңмқҙлӢӨ.
кі м°°
мқјмёЎм„ұ лӮңмІӯ нҷҳмһҗм—җкІҢ м Ғмҡ©н• мҲҳ мһҲлҠ” м№ҳлЈҢ мҳөм…ҳмқҖ CROS мӢңмҠӨн…ң, мқҙмӢқнҳ• кіЁм „лҸ„ ліҙмІӯкё°, мқёкіөмҷҖмҡ° л“ұ лӢӨм–‘н•ңлҚ°[10,11], мқҙ мӨ‘ мқҙмӢқнҳ• кіЁм „лҸ„ ліҙмІӯкё°лҠ” мөңк·ј кі м¶ңл Ҙ м–ҙмқҢмІҳлҰ¬кё°мқҳ к°ңл°ң л°Ҹ лӢӨм–‘н•ң кіЁм „лҸ„ мһ„н”ҢлһҖнҠёк°Җ к°ңл°ңлҗЁм—җ л”°лқј мқјмёЎм„ұ лӮңмІӯ нҷҳмһҗм—җм„ң мЈјмҡ”н•ң м№ҳлЈҢлІ•мқҙ лҗҳкі мһҲлӢӨ.
мқҙлІҲ мҰқлЎҖм—җ мӮ¬мҡ©лҗң Osiaв“Ү2лҠ” нҸүк· кіөкё°м „лҸ„ м—ӯм№ҳ 20 dB HL мқҙн•ҳмқё нҺёмёЎм„ұ к°җк°ҒмӢ кІҪм„ұ лӮңмІӯ, нҸүк· кіЁм „лҸ„ м—ӯм№ҳ 55 dB HL мқҙн•ҳмқё нҳјн•©м„ұ л°Ҹ м „мқҢм„ұ лӮңмІӯ м№ҳлЈҢм—җ лҢҖн•ҙ FDA мҠ№мқёмқ„ л°ӣмқҖ м••м „мһҗк·№ л°©мӢқмқ„ мқҙмҡ©н•ң кіЁм „лҸ„ ліҙмІӯкё°мқҙлӢӨ[9]. м••м „мһҗк·№мқҖ к°Җн•ҙ진 кё°кі„м Ғ 진лҸҷм—җ л°ҳмқ‘н•ҳм—¬ м „н•ҳлҘј мғқм„ұн•ҳкұ°лӮҳ мҷёл¶Җ м „н•ҳм—җ л°ҳмқ‘н•ҳм—¬ кё°кі„м Ғ 진лҸҷмқ„ к°Җм—ӯм ҒмңјлЎң мғқм„ұн•ҳлҠ” нҠ№м • мһ¬лЈҢмқҳ лҠҘл ҘмқҙлӢӨ. л””м§Җн„ё м••м „мһҗк·№мқҖ лҶ’мқҖ м¶ңл Ҙмқ„ м ңкіөн•ҳкі мқҢм„ұ мқҙн•ҙм—җ мӨ‘мҡ”н•ң л¶Җ분мқё лҶ’мқҖ мЈјнҢҢмҲҳм—җм„ң мқҙл“қмқ„ н–ҘмғҒмӢңнӮӨл©°, кё°мЎҙм—җ л§Һмқҙ мӮ¬мҡ©лҗҳлҚҳ лҸҷмқјнҡҢмӮ¬ м ңн’Ҳмқё Bahaв“Ү Attractм—җ 비н•ҙ нҸүк· 9.6 dB, Bahaв“Ү Connectм—җ 비н•ҙ нҸүк· 10.2 dBмқҳ additional gainмқҙ кҙҖм°°лҗҳм—ҲлӢӨ[4,5]. Osiaв“Ү2лҠ” мҲҳлҸҷкІҪн”јл°©мӢқмқҳ BAHA Attract System (Cochlear)мқҙлӮҳ Sophonoв“Ү Alpha 2 MPO (Sophono, Inc., Boulder, CO, USA)ліҙлӢӨ нҡЁмңЁм Ғмқё мҶҢлҰ¬ м „мҶЎ[12]кіј мҶҢлҰ¬к°җмҮ к·№ліө, лҶ’мқҖ мЈјнҢҢмҲҳмқҳ мІӯл Ҙ н–ҘмғҒ[13]мқҙ кё°лҢҖлҗҳл©°, н”јл¶ҖкІҪмң л°©мӢқмқҳ BAHA (Cochlear)лӮҳ Ponto (Oticon Medical, Askim, Sweden)ліҙлӢӨ лҜёмҡ©м ҒмңјлЎң мҡ°мҲҳн•ҳлӢӨ[3,14,15]. Osiaв“Ү2 мқҢн–Ҙ мІҳлҰ¬кё°лҠ” мҶҢлҰ¬ м „мҶЎмқ„ мң„н•ҙ к·№лӢЁм Ғмқё мһҗм„қ к°•лҸ„к°Җ н•„мҡ”н•ҳм§Җ м•Ҡмңјл©°, л¬ҙкІҢ лҳҗн•ң к°ҖліҚкё°м—җ мһҘкё°к°„ мӮ¬мҡ©мӢң н”јл¶Җ мһҗк·№мқҙ м Ғмқ„ кІғмңјлЎң мҳҲмғҒлҗңлӢӨ. лҳҗн•ң, Osiaв“Ү2лҠ” мҷёл¶Җ мһҘм№ҳлҘј нғҲм°©н•ң нӣ„м—җ мЎ°кұҙм ҒмңјлЎң 3-Tesla мқҙн•ҳмқҳ мһҗкё°кіөлӘ…мҳҒмғҒмқ„ мҙ¬мҳҒн• мҲҳ мһҲлӢӨ. л¬јлЎ 3Tмқҳ кІҪмӮ¬ м—җмҪ”(gradient echo)лҘј мӮ¬мҡ© мӢң мқҙлҜём§Җ н—ҲмғҒмқҳ нҒ¬кё°лҠ” мөңлҢҖ м•Ҫ 5 cm м •лҸ„к№Ңм§Җ ліҙкі лҗҳкё°лҠ” н•ҳмҳҖмңјлӮҳ, мҲҳмҲ мқҙнӣ„ 추м Ғ кҙҖм°°мқҙ н•„мҡ”н•ң нҷҳмһҗм—җм„ңлҠ” нҒ° мһҘм җмқҙлқј мғқк°Ғн•ңлӢӨ.
ліё мҰқлЎҖл“ӨмқҖ мҲҳмҲ м „ мҲңмқҢмІӯл ҘкІҖмӮ¬м—җм„ң 100 dB HL мқҙмғҒмқҳ мІӯл Ҙм—ӯм№ҳк°Җ к°Ғк°Ғ 21 dB HL, 41 dB HLлЎң 80 dB HL, 60 dB HLм”© н–ҘмғҒлҗҳм—Ҳкі K-HINT м җмҲҳмғҒ мЎ°мҡ©н•ҳкі мӢңлҒ„лҹ¬мҡҙ нҷҳкІҪ лӘЁл‘җм—җм„ң Osiaв“Ү2 м°©мҡ© мӢң нҡЁкіјк°Җ мһҲмқҢмқ„ нҷ•мқён• мҲҳ мһҲм—ҲлӢӨ.
Osiaв“Ү2лҠ” м••м „ нҡЁкіјлҘј нҷңмҡ©н•ң лҠҘлҸҷнҳ• мІӯк°Ғ кіЁмңөн•© мһ„н”ҢлһҖнҠёлЎң лҶ’мқҖ м¶ңл Ҙмқ„ м ңкіөн•ҳкі н–ҘмғҒлҗң кі мЈјнҢҢ мқҙл“қмқ„ м ңкіөн•ҳм—¬ мқҢм„ұ мқёмӢқмқ„ мөңм Ғнҷ”н•ҳлҠ” лҸҷмӢңм—җ нҺём•Ҳн•Ёкіј лҜёмҡ©м Ғмқё мёЎл©ҙм—җм„ңлҸ„ к°ңм„ лҗҳм—Ҳмңјл©° мқҙлҘј кё°л°ҳмңјлЎң лҶ’мқҖ нҷҳмһҗ л§ҢмЎұлҸ„лҘј м ңкіөн•ңлӢӨ. ліё мҰқлЎҖмҷҖ к°ҷмқҙ мІӯл Ҙ к°ңм„ мқҳ нҡЁкіјмҷҖ лҜёмҡ©м Ғмқё мһҘм җ, мӮ¬мҡ©мқҳ мҡ©мқҙм„ұмқ„ кі л Өн•ҙ ліёлӢӨл©ҙ 추нӣ„м—җлҸ„ 비мҠ·н•ң мң нҳ•, мҰү мҲҳмҲ мқҙнӣ„ л°ңмғқн•ң мқјмёЎм„ұ лӮңмІӯ нҷҳмһҗм—җм„ң Osiaв“Ү2 мқҙмӢқмқҙ мўӢмқҖ мІӯк°Ғмһ¬нҷңл°©лІ•мқҙ лҗ кІғмңјлЎң мғқк°ҒлҗңлӢӨ.