서 론
최근 청각 기능의 결손이 치매의 위험 요인으로 주목받게 되면서[1] 청각 검사를 치매 진단에 활용하고자 하는 일련의 연구들이 활발히 진행되고 있다[2]. 구체적으로, 알츠하이머병(Alzheimer’s disease, AD) 환자에게 청성유발전위(auditory event-related potentials)의 여러 요소들 중 N200과 P300 측정 파형의 잠복기(latency)와 P300 반응의 진폭(amplitude)을 분석한 결과들을 바탕으로 메타 분석을 실시한 연구에서는 정상 인지 기능의 대조군과 비교 시 AD 환자의 N200과 P300 잠복기가 유의하게 지연되었고[3,4] P300의 진폭은 유의하게 감소하였다[5]. 이러한 선행 연구들은 임상 적용을 위한 기초적 자료제공은 가능하지만, 대부분의 개별 연구에서 한계점으로 보고하였듯이 특정 요소의 측정 반응에만 초점을 두어 아쉽게도 청각적 정보처리 및 인지 과정을 종합적으로 파악하지 못하였다[6]. 즉, 청각 기관을 통한 선택적 주의력(selective attention)과 관련 있는 N100, 소리의 음향적 특성 분석의 기초 능력(elementary feature analysis)과 연관된 N200, 청각 정보 처리 및 청각적 인지 기능을 측정하는 P300 등 여러 요소들의 결과들을 근거로 중추청각기관의 경로를 전반적으로 확인하고 치매 환자들의 청각 처리 능력을 종합적으로 이해할 필요가 있다[7].
대표적으로 알려진 퇴행성 뇌 질환은 AD, 파킨슨병(Parkinson’s disease, PD), 루이소체치매(dementia with Lewy bodies, DLB), 파킨슨병치매(Parkinson’s disease dementia, PDD) 등으로, 공통적으로 변형된 단백질의 비정상적 침착으로 인한 변형단백질환(proteinopathy)을 특징으로 한다. 그러나 퇴행성 뇌질환으로 인한 치매는 한 종류의 변형 단백질로 야기된 문제보다는 여러 변형 단백질들의 복합적인 영향을 받게 되기에, 유형이 다른 치매들 간에도 증상이 비슷하게 나타나는 경우가 흔하다[8]. 예를 들어, 사후 부검 연구에서는 일부 DLB 환자에서 베타-아밀로이드가 검출되기도 하고, 역으로 후기 AD 환자에서는 알파-시누클레인의 변형된 형태인 루이소체(Lewy body, LB)가 관찰되기도 한다[9]. 특히, AD, DLB, PDD는 그 형태가 많이 중복되기에 진단에 어려움이 있으며, 이들의 관계를 밝히기 위한 연구가 계속해서 진행되고 있다[8]. 1995년에 DLB는 AD와 PDD로 부터 임상병리학적으로 구분이 되었으나, 2014년까지도 DLB를 다른 유형의 치매로 오진하는 경우가 많아 최근에도 계속해서 진단 기준이 수정되고 있다[10].
Hardy 등[11]은 치매의 유형에 따른 피질의 구조적 또는 위치적 손상이 청각 기능 저하에 정도의 차별적 영향을 줄 수 있다고 보고하였다. 즉, 치매는 청각 기능이 비교적 잘 보존되는 유형이 있는 반면, 심각한 청각 기능 손상을 보이는 치매의 유형이 있다. 청각적 기능 손상과 관련된 뇌 네트워크의 병리학적 위치를 구분해보면, AD 환자의 경우 후측대상피질(posterior cingulate cortex), 쐐기앞소엽(precuneus), 측두두정부(temporo-parietal cortices)로[11], 해당 위치의 손상은 복잡한 음향 환경에서 음원의 위치를 파악하는 능력이 저하되며[12] 청각장면분석(auditory scene analysis)이 어려워지고[13] 소리에 대한 민감도가 증가하게 된다[14]. 반면, DLB와 PDD의 의병리학적 위치는 피질-피질하 회로(cortico-subcortical circuits)로써 해당 부위의 손상은 청각적 자극에 대한 탐지 및 분석이 어렵고 청각장면분석 능력이 저하되어[15,16] 궁극적으로는 청각적 주의력과 작업 기억력에 부정적 영향을 끼치게 된다[17]. 이러한 다양한 치매 유형들의 청각 기능의 차이에 따라 청각 검사를 환자들에게 적용하여 그 유형을 세분화하고자 하는 연구들이 시도되고 있으나[18-20], 실제 임상 현장의 적용까지는 많은 검증이 필요한 상황이다.
치매 환자의 청각 검사 결과들을 바탕으로 실시한 기존의 메타 분석 연구는 다음과 같은 한계점을 갖는다. 청성유발전위 검사들 중 특정 요소만의 메타 분석 결과를 제공했고, 1995년 이전 문헌을 포함하여 치매 유형에 따른 연구 대상자를 구분하지 못하였을 가능성이 높고, 치매 환자의 주관적 측정 결과에 대한 메타 분석 문헌의 부재 등이다. 따라서 본 종설 논문에서는 비교적 비슷한 증상으로 진단이 까다로운 AD, DLB, PDD 환자들에게 객관적 및 주관적으로 실시한 청각 검사들을 적용한 문헌들을 검색하고 세분화하여 분류한 후 메타 분석을 실시하여 현재 치매 환자들의 청각 결과들을 종합적으로 정리하고자 한다.
본 론
체계적 문헌 검색의 전략과 선정
문헌 선정, 데이터 추출과 분석, 문헌의 포함과 제외 방법은 Participants, Index test, Control, Outcomes, Study design (PICOS) 기준을 적용하였다[21]. 즉, 문헌은 PICOS 기준에 의거하여 선정 및 분류되었으며, 구체적인 체계적 문헌 고찰의 과정은 PRISMA 2015 Flow Diagram을 참고하여 작성하였다[22]. 체계적 문헌 고찰의 모든 과정은 두 명의 저자에 의해 독립적으로 평가되었다. 추출된 데이터 및 문헌이 두 저자에 의해 합의가 이루어지지 않은 경우에는 문헌을 재검토하여 논의하였다. 본 연구에 적용한 PICOS 기준은 Table 1에 기술하였다.
문헌 발견(Identification)
본 종설에서는 AD, DLB, PDD 환자군을 대상으로 청각 검사를 적용한 연구만을 선정하고 수집하였다. 연구 목적에 따른 구체적인 문헌 선정을 위해, 7개의 전문 학술 전자 데이터베이스인 Pubmed, Embase, Medline, Web of science, SciELO, Scopus, Cochrane Library에서 문헌을 검색하였다. 검색어는 의학주제명표목(Medical Subject Headings, MeSH) 용어 및 선행 문헌에서 자주 표현된 용어에서 확인하였다: ‘Alzheimer disease(AD)’ OR ‘Parkinson’s disease Dementia (PDD)’ OR ‘Dementia with Lewy bodies(DLB)’ OR ‘Proteinopathy’ OR ‘Lewy’ OR ‘Dementia’ OR ‘Alzheimer’ AND ‘Auditory function’ OR ‘Biomarker’ OR ‘Auditory perception’ OR ‘Speech perception’ OR ‘Electroencephalography (EEG)’ OR ‘Speech recognition’ OR ‘Evoked potential’ OR ‘Event-related potential’ OR ‘Electrophysiology’ OR ‘Auditory stimulation’ OR ‘Behavioral’ OR ‘Objective’ AND ‘Pure tone audiometry(PTA)’ OR ‘Mismatch negativity (MMN)’ OR ‘P300(P3)’ OR ‘N100(N1)’ OR ‘N200(N2)’ OR ‘P100(P1)’ OR ‘N400(N4)’ OR ‘Auditory brainstem response (ABR)’ OR ‘Otoacoustic emission(OAE)’ OR ‘Auditory steady-state response(ASSR)’ OR ‘Auditory middle latency response(AMLR)’.
출간기간에 따른 문헌들의 선정기준은 The Consortium on Dementia with Lewy bodies에서 DLB의 진단기준을 설정하고 별개의 임상 증후군으로 인정되어 DLB가 AD 및 PDD와의 임상 병리학적 분리가 구체화된 1995년 1월을 기점으로 하였다[23]. 즉, 1995년 1월~2020년 5월까지의 문헌이 본 논문에 포함되었다. 본 종설에서는 연구논문만을 포함하여 서적, 종설, 학회 초록, 메타 분석 연구는 제외되었으며, 경도인지장애 및 동물 연구 또한 제외시켰다.
문헌 선별(Screening)
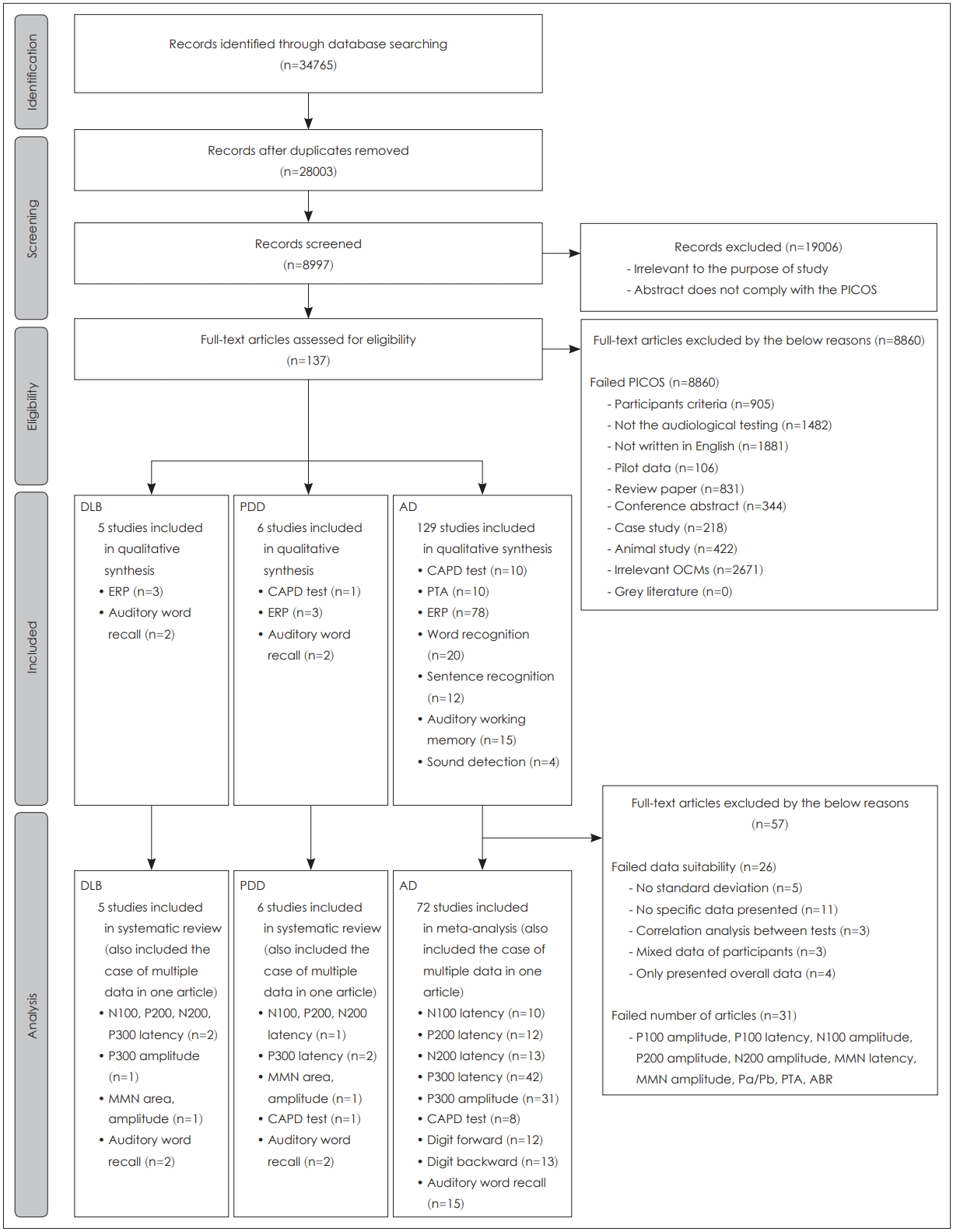
7개의 전문 학술 전자 데이터베이스를 사용하여 34765개의 문헌이 검색되어 스크리닝 단계에 포함되었다(Fig. 1, Identification level). 그 중 중복되는 문헌(n=6762)을 제거하여 28003개의 문헌이 선별되었고, 문헌의 초록을 PICOS 기준에 의거하여 두 명의 저자에 의해 독립적으로 검토되었다. 결과적으로 19006개의 문헌이 제거되어 총 8997개의 문헌이 선정기준 평가 단계에 포함되었다(Fig. 1, Screening level). 즉, 선정기준 평가 단계에 포함된 문헌들은 PICOS 기준을 충족하거나, 초록의 내용만으로는 평가하기 어려운 경우를 모두 포함하였다.
선정 기준(Eligibility)의 검토 및 최종 선정(Inclusion)
다양한 이유로 PICOS 기준을 충족하지 못한 8860개의 문헌이 제거되어, 결과적으로 137개의 문헌이 선정기준에 만족하였다(Fig. 1, Eligibility level). 그 중 129개의 문헌이 AD 환자군을 포함하였으며, DLB와 PDD 환자군을 포함한 문헌은 각각 5개와 6개였다(Fig. 1, Included level). 해당 문헌에서 주로 사용된 청각 검사들은 청성유발전위 검사, 중추청각검사, 청각단어회상검사, 순음청력검사, 단어인지검사, 문장인지검사 등이다.
AD 환자군을 포함한 개별 문헌에서 데이터를 추출하는 과정 중 표준편차 데이터 누락(5/26), 구체적인 수치의 누락(11/26), 검사 도구간의 상관 분석 결과만을 제시하여 고유의 데이터 확인이 불가(3/26), 연구대상자 간의 혼재된 결과 제시(3/26), 전체적인 데이터만을 제시한(4/26), 총 26개의 문헌이 추가적으로 제거되었다. 데이터의 추출 과정에서 선정기준을 만족하였으나, 포함된 문헌 수가 6개 이하로 매우 적어 메타 분석에 포함되지 못한 검사는 P100 진폭, P100 잠복기, N100 진폭, P200 진폭, N200 진폭, mismatch negativity (MMN) 잠복기, MMN 진폭, Pa/Pb, puretone audiometry (PTA), auditory brainstem response(ABR)였으며, 총 31건의 문헌이 이에 포함되었다. 따라서, 메타 분석을 실시하기 위해 최종 72개의 문헌이 포함되었다(Fig. 1, Analysis level).
AD 환자의 청각 기능에 관한 메타 분석
메타 분석에 사용된 문헌은 AD 환자의 청각 검사 결과, 실험군과 동일 연령의 대조군 결과, 적절한 결과 측정 데이터를 모두 포함하였다. 효과 크기의 계산은 실험군과 대조군의 평균, 표준편차, 연구대상자의 수를 사용하였고, 청성유발전위 반응 및 청각적 수행력을 확인한 실험 결과임에도 대부분의 연구는 검사 설정 및 검사 도구의 다양성으로 인해 표준화된 평균 차이(standardized mean difference, SMD)로 효과 크기가 계산되었다[24]. 모든 효과 크기는 95%의 신뢰구간을 갖는 확률효과모델(random effect model)을 사용하였으며, 하위군 분석은 하위군 간의 혼합 효과 Q검정을 사용하여 효과 크기를 비교하였다[25]. 하나의 문헌에서 여러개의 데이터가 추출될 경우 각각의 데이터는 개별적인 데이터로 간주하여 분석을 실시하였다. 예를들어, 하나의 문헌에서 특정 요소의 반응을 다양한 전극위치에서 확인할 때 각각의 결과는 개별 데이터로 간주된다. 전극위치는 같지만 자극음에 따른 반응을 측정한 경우에도 자극음에 따른 각각의 반응 결과가 개별 데이터로 간주된다. 깔때기 도표(funnel plot)와 Egger’s 회귀 비대칭 분석은 출판편향(publication bias)을 확인하기 위해 사용되었다[26]. 메타 분석을 위해 Comprehensive MetaAnalysis (Ver. 3, Biostat Inc., Englewood, NJ, USA) 프로그램을 사용하였다.
본 메타 분석에 사용된 72개의 문헌들의 데이터를 바탕으로 Fig. 2를 제작하여 AD 환자군과 대조군의 각 검사별 차이값을 가시화하였다. 메타 분석 및 Egger’s 회귀 비대칭 분석의 결과는 Table 2에 정리하였다. 대부분의 메타 분석 결과에서 높은 이질성(I2≥75%)이 확인되어 청성유발전위 검사는 측정 전극과 자극음의 종류를 구분하여 하위군 분석을 실시하였다. 또한, 주관적 청각검사에서는 검사 도구의 종류, 검사의 특성을 고려하여 지연시간, 측정한 귀에 대해 하위군 분석을 실시하였다. 메타 분석의 숲 그림(forest plot)은 부록(Appendix 1, 2, and 3)에 제시하였다.
객관적 청성유발전위 검사
N100 latency
N100 잠복기의 메타 분석은 12개의 문헌에서 총 15개의 데이터로 실시하였다. 15개의 데이터 평균은 다른 측정 요소들과 함께 Fig. 2A에 제시하였다(AD mean: 107.15±10.74 ms, control mean: 107.00±14.59 ms). AD 환자군과 대조군의 N100 잠복기를 비교한 메타 분석 결과는 유의한 차이를 보이지 않았으며[SMD=0.672, 95% confidence interval(CI)=-0.051 to 1.395, p=0.069], 높은 이질성이 확인되었다(I2=94.15%). Egger’s 회귀 비대칭 분석시 출판편향이 존재함을 확인하였다[intercept=12.199, standard error(SE)=3.047, p<0.001]. 높은 이질성으로 인해 측정 전극에 대해 하위군 분석을 실시하였으나, 자극음의 종류는 포함된 15개의 데이터가 1000 Hz의 배경음, 2000 Hz의 목표음으로 동일하여 하위군 분석을 실시하지 않았다.
전극 위치에 따른 하위군 분석 후에도, 여전히 높은 이질성이 관찰되었다(SMD=1.973, 95% CI=0.626 to 3.321, p=0.004; I2=93.37%). 하위군 분석에 포함된 15개 데이터의 전극 위치(데이터수)는 Cz(8/15), Fz(2/15), Oz(1/15), Pz(4/15)였고, 주요 전극 위치의 효과 크기는 Oz(SMD=4.366, 95% CI=1.799 to 6.933, p<0.001), Fz(SMD=2.621, 95% CI=0.845 to 4.397, p=0.004), Pz(SMD=1.366, 95% CI=0.136 to 2.596, p=0.030), Cz(SMD=0.885, 95% CI=0.012 to 1.759, p=0.047)의 순으로 확인되어 Oz 위치에서 AD 환자군과 대조군의 N100의 잠복기 차이가 상대적으로 가장 컸다.
P200 latency
P200 잠복기에 관한 메타 분석은 10개의 문헌에서 총 15개의 데이터를 추출하여 수행하였다. 포함된 15개의 데이터 평균은 Fig. 2A에 제시하였다(AD mean: 200.19±15.99 ms, control mean: 187.43±12.21 ms). Egger’s 회귀 비대칭 분석 결과에서 출판편향이 존재하지 않았지만(intercept=-0.678, SE=2.423, p=0.392), 종합적인 메타 분석의 결과는 유의한 차이를 확인할 수 없었고(SMD=0.129, 95% CI=-0.131 to 0.389, p=0.331), 중간크기의 이질성이 확인되어(I2=61.33%) 하위군 분석을 측정 전극 및 자극음의 종류에 대해 실시하였다.
하위군 분석에 포함된 15개의 전극 위치(데이터수)는 C5(1/15), C6(1/15), Cz(8/15), Fz(1/15), Pz(4/15)였으며, 자극 음의 종류는 1000/2000(12/15)와 250/4000(2/15)의 배경음/목표음(데이터수), 800 Hz 단일 자극음(1/15)이었다. 전극 위치에 따른 하위군 분석의 결과로 어느 정도 이질성이 해결되었으나, 여전히 중간크기의 이질성이 확인되었다(SMD=0.134, 95% CI=-0.173 to 0.440, p=0.394; I2=55.69%). 하위군 분석 으로 확인된 효과 크기는 C5(SMD=4.366, 95% CI=-0.529 to 1.396, p=0.377), Pz(SMD=0.307, 95% CI=-0.160 to 0.775, p=0.197), Fz(SMD=0.214, 95% CI=-0.775 to 1.203, p=0.671), Cz(SMD=0.015, 95% CI=-0.336 to 0.365, p=0.935), C6(SMD=-0.253, 95% CI=-1.212 to 0.707, p<0.001)의 측정 전극 순이였다. C5 위치에서 P200의 잠복기 차이가 비교적 컸으나 통계적으로 유의한 차이를 보여주지는 않았다. 또한, 해당 위치에서 측정된 데이터의 개수는 1개로 다른 전극 위치와의 직접적인 효과크기 비교가 어려웠다.
자극음에 따른 하위군 분석 또한 이질성이 어느 정도 해결이 되었으나, 중간 크기의 이질성이 확인되었다(SMD=0.069, 95% CI=-0.285 to 0.424, p=0.702; I2=55.69%). 1000/2000 Hz 집단에서 가장 큰 효과 크기를 보였으며(SMD=0.185, 95% CI=-0.081 to 0.452, p=0.173), 그 다음으로 250/4000 Hz의 자극음 집단(SMD=0.089, 95% CI=-0.549 to 0.728, p=0.784), 800 Hz 단일 자극음 집단 순으로 확인되었으나 모두 통계적으로 유의하지 않았다(SMD=-0.415, 95% CI=-1.234 to 0.403, p=0.320).
N200 latency
N200 잠복기의 메타 분석은 13개의 문헌에서 총 16개의 데이터를 추출 후 실시하였다. 추출된 16개의 데이터의 평균은 Fig. 2A에 제시되었다(AD mean: 283.05±31.66 ms, control mean: 246.85±20.45 ms). Egger’s 회귀 비대칭 분석에서 출판편향이 나타났다(intercept=6.772, SE=2.586, p=0.010). 전반적으로 N200 잠복기에 유의한 차이를 보였으나(SMD=1.144, 95% CI=0.475 to 1.813, p<0.001), 높은 이질성으로 인해 전극 위치에 따른 반응의 잠복기를 하위군 분석으로 실시하였다(I2=92.73%). 포함된 16개의 데이터는 모두 배경음 1000 Hz, 목표음 2000 Hz을 사용하였다.
하위군 분석에 사용된 16개의 데이터(데이터수)는 Cz(9/16), Pz(2/16), Fz(5/16)의 전극위치에서 측정되었으며, 하위군 분석을 진행하였음에도 높은 이질성이 확인되었다(SMD=1.930, 95% CI=0.594 to 3.267, p=0.005; I2=90.97%). 각 하위군의 효과 크기는 Fz(SMD=3.281, 95% CI=1.539 to 5.023, p<0.001), Pz(SMD= 2.084, 95% CI=1.027 to 3.141, p<0.001), Cz(SMD=0.911, 95% CI=0.131 to 1.691, p=0.022)의 순으로 나타나, Fz 위치에서 측정한 N200의 잠복기가 AD 환자군과 대조군 간의 차이를 명확하게 보여주는 것으로 확인되었다.
P300 latency
P300 잠복기의 메타 분석은 42개의 문헌이 포함되었으며, 총 69개의 데이터가 사용되었다. 포함된 69개의 데이터 평균은 다른 측정 요소와 함께 Fig. 2A에 제시하였다(AD mean: 410.22±40.80 ms, control mean: 366.46±25.98 ms). P300 잠복기의 메타 분석 결과에서는 유의한 차이가 확인되었지만(SMD=1.220, 95% CI=0.936 to 1.504, p<0.001), 이질성 또한 높게 확인되었다(I2=91.50%). 출판편향도 존재하였기에(intercept=6.089, SE=1.067, p<0.001), 자극음 종류와 전극 위치에 따른 하위군 분석을 진행하였다.
하위군 분석을 실시하여 어느 정도 이질성이 해결되었지만, 이질성은 여전히 높았다[전극위치: (SMD=1.315, 95% CI=0.758 to 1.872, p<0.001; I2=86.52%), 자극음: (SMD=0.960, 95% CI=0.261 to 1.659, p=0.007; I2= 86.52%)]. 전극 위치에 따른 하위군 분석에 포함된 69개의 데이터 중에서 문헌에서 주로 사용된 전극(데이터수)인 Cz(26/69), Fz(15/69), Pz(25/69)의 결과를 바탕으로 비교하였다. 전극 위치에 따른 효과 크기는 Pz(SMD=1.332, 95% CI=0.974 to 1.690, p<0.001), Fz(SMD=1.096, 95% CI=0.745 to 1.446, p<0.001), Cz(SMD=1.332, 95% CI=0.974 to 1.690, p<0.001) 순으로 나타나 Pz의 전극 위치에서 AD 환자군과 대조군 간의 P300 잠복기의 차이가 가장 크게 확인되었다.
자극음에 따른 하위군 분석에 포함된 데이터의 자극음 종류(데이터수)는 1000/2000 Hz(57/69), 1601/402 Hz(1/69), 250/4000 Hz(1/69), 500/1000 Hz(3/69), 750/2000 Hz(3/69), 980/1970 Hz(1/69), 숫자(1/69), 자극음 데이터 없음(2/69)으로 다양했다. 각 자극음 하위 그룹의 효과 크기는 다음과 같다: 1000/2000 Hz(SMD=1.334, 95% CI=1.089 to 1.580, p<0.001), 1601/402 Hz(SMD=0.450, 95% CI=-1.479 to 2.380, p=0.647), 250/4000 Hz(SMD=0.887, 95% CI=-0.916 to 2.690, p=0.335), 500/1000 Hz(SMD=0.410, 95% CI=-0.630 to 1.451, p=0.439), 750/2000 Hz(SMD=1.236, 95% CI=0.210 to 2.263, p=0.018), 980/1970 Hz(SMD=-1.189, 95% CI=-3.106 to 0.728, p=0.224), 숫자(SMD=3.687, 95% CI=1.276 to 6.097, p=0.003), 자극음 데이터 없음(SMD=1.108, 95% CI=-0.162 to 2.378, p=0.087).
P300 amplitude
P300 진폭의 메타 분석은 31개의 문헌에서 총 56개의 데이터가 포함되었다. 56개의 데이터의 평균은 Fig. 2B에 제시하였다. 대조군(8.69±3.54 μV)에 비해 AD 환자군의 P300 진폭평균은 6.39±3.48 μV로 작았다. 메타 분석 결과, P300 진폭의 유의한 차이가 확인되었으나(SMD=-0.595, 95% CI=-0.907 to -0.284, p<0.001) 높은 이질성이 확인되었고(I2=91.63%), 출판편향 또한 존재하였다(intercept=-6.934, SE=1.576, p<0.001). P300의 진폭 역시 높은 이질성으로 인해 전극 위치와 자극음의 하위군 분석을 실시하였다.
하위군 분석 실시 후에도 여전히 높은 이질성이 관찰되었다[전극위치: (SMD=-1.036, 95% CI=-1.594 to -0.477, p<0.001; I2=88.15%), 자극음: (SMD=-0.844, 95% CI=-1.526 to-0.162, p=0.015; I2=88.15%)]. 전극 위치에 따른 하위군 분석으로 C3(SMD=-2.922, 95% CI=-5.025 to -0.819, p=0.006), C4(SMD=-2.658, 95% CI=-4.733 to -0.584, p=0.012), FCz(SMD=-0.468, 95% CI=-2.423 to 1.486, p=0.639), Oz(SMD=-2.733, 95% CI=-4.648 to -0.818, p=0.005)는 각각 한 개의 데이터만이 추출되어 분석되었음으로 직접적인 비교가 어려웠다. 따라서, 전극 위치(데이터수)는 Cz(19/56), Fz(12/56), Pz(21/56)의 결과가 비교되었다. 전극 위치에 따른 효과 크기는 Cz(SMD=-0.698, 95% CI=-1.135 to -0.261, p=0.002), Pz(SMD=-0.696, 95% CI=-1.110 to -0.283, p<0.001), Fz(SMD=-0.593, 95% CI=-1.139 to -0.047, p=0.033)의 순으로 확인되어, Cz의 전극 위치에서 AD 환자군과 대조군 간의 P300 진폭의 차이가 가장 크게 나타났다.
자극음 하위군 분석에 포함된 데이터(데이터수)는 1000/2000 Hz(43/56), 250/4000 Hz(1/56), 500/1000 Hz(2/56), 750/2000 Hz(3/56), 800/1200 Hz(3/56), 980/1970 Hz(1/56), 자극음 데이터 없음(3/56)이었다. 하위군 분석의 효과 크기 결과는 1000/2000 Hz(SMD=-0.736, 95% CI=-1.036 to-0.436, p<0.001), 250/4000 Hz(SMD=-0.240, 95% CI=-2.166 to 1.686, p=0.807), 500/1000 Hz(SMD=-0.633, 95% CI=-2.010 to 0.745, p=0.368), 750/2000 Hz(SMD=-0.217, 95% CI=-1.315 to 0.881, p=0.699), 800/1200 Hz(SMD=-2.722, 95% CI=-3.957 to -1.487, p<0.001), 980/1970 Hz(SMD=-0.468, 95% CI=-2.484 to 1.548, p=0.649), 자극음 데이터 없음(SMD=-0.636, 95% CI=-1.748 to 0.476, p=0.262) 이었다.
주관적 중추청각행동검사
중추청각장애검사 배터리
중추청각장애검사는 8개의 문헌이 포함되어 총 20개의 데이터가 메타 분석에 사용되었다. 20개의 데이터 평균은 Fig. 2C에 제시하였다(AD mean: 61.20±20.15%, control mean: 90.03±10.41%). 흥미롭게도, Fig. 2D에서는 AD 환자군의 우측 귀 수행력이 66.36±19.78%였으며, 대조군은 90.49±11.58%의 수행력을 보였다. 좌측 귀 수행력의 평균은 AD 환자군이 55.39±22.46%였고, 대조군은 91.15±10.32%로, AD 환자군은 좌측 귀 수행력이 우측귀에 비해 약 10% 낮았다. 양측 귀의 수행력 평균은 AD 환자군이 58.70±10.60%, 대조군이 83.30±1.41%로 확인되었다.
메타 분석 결과에서 유의한 차이가 확인되었으며(SMD=-1.299, 95% CI=-1.512 to -1.086, p<0.001), 이질성도 낮았다(I2=13.49%). 출판편향은 존재하는 것으로 확인되었다(intercept=-3.461, SE=0.700, p<0.001). 메타 분석에 포함된 데이터(데이터수)의 검사는 이분숫자청취(dichotic digits)(6/20), 이분문장청취(dichotic sentence)(2/20), 음장단패턴(duration pattern)(1/20), 주파수패턴(pitch pattern)(1/20), Synthetic Sentence Identification message-to-competition ratios(SSI/MCR) +10(2/20), SSI/MCR 0(2/20), SSI/MCR -10(2/20), SSI/MCR -20(2/20), Synthetic Sentence Identification test with contralateral competing message(1/20), Synthetic Sentence Identification test with ipsilateral competing message(1/20)이 포함되었으며, 수행력을 측정한 귀(데이터수)는 양측(2/20), 좌측(8/20), 우측(10/20)이었다.
숫자 폭(Digit span) 검사
숫자 바로 따라하기(digit span forward)의 메타 분석에 포함된 문헌은 12개였다. 포함된 12개의 데이터 평균은 AD 환자군이 6.09±0.52였고, 대조군이 7.08±0.80이었다(Fig. 2E). 숫자 바로 따라하기의 메타 분석 결과에서 유의한 차이가 확인되었고(SMD=-0.659, 95% CI=-0.918 to -0.399, p<0.001), 중간크기의 이질성이 확인되었다(I2=42.59%). 한편, 출판편향은 존재하지 않는 것으로 확인되었다(intercept=-2.997, SE=2.715, p=0.148). 하위군 분석은 검사 종류에 대해 실시되었으며, 검사 종류(데이터수)는 웩슬러 지능 검사(Wechsler Adult Intelligence Scale-Revised, WAIS-R)(6/12)의 정량화된 결과와 최대 숫자 수행력(6/12)이 하위군으로 포함되었다.
검사 종류에 따른 하위군 분석 결과는 포함된 문헌의 숫자 바로 따라하기 수행력에서 각각 한 개씩의 데이터만 보고되어 이질성 결과는 동일하였다(SMD=-0.660, 95% CI=-0.926 to -0.394, p<0.001; I2=42.59%). 하위군의 개별적인 결과에서 효과 크기의 차이는 상대적으로 WAIS-R이 높았으며(SMD=-0.747, 95% CI=-1.135 to -0.358, p<0.001), 상당히 낮은 이질성을 보였다(I2=2.53%). 반면, 최대 숫자 수행력은 높은 이질성을 보였다(SMD=-0.583, 95% CI=-0.949 to -0.218, p=0.002; I2=61.96%).
숫자 거꾸로 따라하기(digit span backward)의 메타 분석에 포함된 문헌은 13개이다. 포함된 13개 데이터의 평균은 AD 환자군이 4.06±0.59, 대조군이 5.37±0.72였다(Fig. 2E). 출판편향은 없는 것으로 확인되었으며(intercept=-4.315, SE=2.510, p=0.057), 메타 분석 결과는 유의한 차이가 확인되었고 중간크기의 이질성이 확인되었다(SMD=-0.901, 95% CI=-1.179 to -0.624, p<0.001; I2=51.71%). 검사종류(데이터수)에 따른 하위군 분석을 위해 WAIS-R(6/13), 최대 숫자 수행력(7/13)이 하위군으로 포함되었다. 하위군 분석의 이질성은 숫자 바로 따라하기와 동일하였다(SMD=-0.904, 95% CI=-1.190 to -0.617, p<0.001; I2=51.71%). 분석 결과, WAIS-R의 효과 크기가 최대 숫자 수행력을 확인한 효과 크기보다 상대적으로 더 크게 나타났다[WAIS-R: (SMD=-0.983, 95% CI=-1.419 to -0.548, p<0.001; I2=42.01%), 최대 숫자 수행력: (SMD=-0.843, 95% CI=-1.223 to -0.462, p<0.001; I2=61.65%)].
청각 단어 회상(Auditory word recall) 검사
청각 단어 회상 검사의 메타 분석은 15개의 문헌에서 총 23개의 데이터가 포함되었다. 추출된 23개의 데이터 평균은 AD 환자군이 3.52±6.70이었으며, 대조군은 9.06±8.08를 보였다(Fig. 2F). 메타 분석 결과, 청각 단어 회상과제의 유의한 차이가 확인되었으나(SMD=-2.308, 95% CI=-2.767 to -1.848, p<0.001) 높은 이질성이 확인되었으며(I2=95.87%), 출판편향 또한 존재하였다(intercept=2.671, SE=1.538, p<0.048). 높은 이질성으로 인해 회상에 대한 지연시간과 검사도구의 하위군 분석을 실시하였다.
하위군 분석을 실시하여 이질성이 일부 해결되었지만, 여전히 이질성은 높게 나타났다[회상에 대한 지연시간: (SMD=-2.267, 95% CI=-3.264 to -1.269, p<0.001; I2=91.96%), 검사도구: (SMD=-1.880, 95% CI=-2.911 to -0.850, p<0.001;I2=91.96%)]. 회상에 대한 지연시간(데이터수)에 따른 하위군 분석으로 하위군은 구체적인 시간을 기재하지 않은 지연회상(8/23), 즉시회상(3/23), 장기지연회상(6/23), 단기지연회상(6/23)의 총 23개의 데이터가 포함된 4개의 군으로 나뉘었다. 개별 집단의 효과 크기는 장기지연회상(SMD=-3.277, 95% CI=-3.717 to -2.837, p<0.001), 단기지연회상(SMD=-3.257, 95% CI=-3.697 to -2.818, p<0.001), 지연회상(SMD=-2.296, 95% CI=-2.745 to -1.846, p<0.001), 즉시회상(SMD=-0.222, 95% CI=-0.973 to 0.529, p=0.563)순으로 확인되었다.
하위군 분석에 포함된 검사도구의 종류(데이터수)는 캘리포니아 언어 학습 검사(California Verbal Learning Test, CVLT) (5/23), 레이 청각 언어 학습 검사(Rey Auditory Verbal Learning Test, RAVLT)(2/23), 청각 언어 학습검사(Auditory-Verbal Learning Test, AVLT)(11/23), 필라델피아 언어 학습 검사(Philadelphia Verbal Learning Test, PVLT)(1/23), 웩슬러지능 검사(2/23), Battery of Cognitive Assessment Instruments developed by World Health Organization(WHOBCAI)(2/23)이었다. 각 검사에 대한 효과 크기는 청각 언어 학습검사(SMD=-2.953, 95% CI=-3.216 to -2.691, p<0.001), 캘리포니아 언어 학습 검사(SMD=-3.451, 95% CI=-3.927 to -2.975, p<0.001), 필라델피아 언어 학습 검사(SMD=3.381, 95% CI=2.068 to 4.694, p<0.001), 레이 청각 언어 학습검사(SMD=-1.884, 95% CI=-2.645 to -1.123, p<0.001), 웩슬러지능 검사(SMD=-1.511, 95% CI=-2.281 to -0.741, p<0.001), WHO-BCAI(SMD=-2.299, 95% CI=-2.951 to -1.646, p<0.001)로 확인되었다.
DLB 환자의 청각 기능을 위한 체계적 연구 결과 분석
DLB 환자들을 대상으로 청각 검사를 실시한 문헌은 대상자가 중복된 문헌을 포함하여 5개로 확인되었다. 문헌의 수의 부족과 검사 도구의 이질성으로 인해 메타 분석의 실시가 불가능하여 체계적 연구 결과 분석을 실시하였고 해당 문헌에 대한 자세한 내용은 Table 3에 요약하여 정리하였다.
객관적 청각유발전위 검사
Bonanni 등[18]은 초기 AD 환자와 DLB 환자의 차이를 청성후기반응(N100, P200, N200, P300)을 통해 확인하였다. 연구 대상자로는 AD와 DLB 환자군과 정상 인지를 지닌 노인 대조군이 포함되었다. 연구의 결과는 N100과 P200간의 잠복기, 진폭간의 차이는 확인할 수 없었고, N200과 P300간의 잠복기는 세개의 집단간 유의미한 상관관계가 나타났다(r=0.6~0.7). 대조군의 결과를 기준으로 적용한 P300의 상대적 잠복기의 지연비율은 Fz와 Cz위치에서 DLB환자 비율이 AD 환자 비율보다 높았으며, 통계적으로 유의한 결과를 보였다[(Fz=AD: 55%, DLB: 92%, p<0.01), (Cz=AD: 49%, DLB: 85%, p<0.01)]. 전두부에서 후두부로의 진폭 분포 변화(AD=3%, DLB=77%, p<0.001)와 후두부에서 전두부로의 진폭 분포 변화(AD=36%, DLB=0%, p<0.01)도 통계적으로 유의한 결과를 보였다. 대조군과 AD 환자군의 P300 반응의 진폭은 Pz에서 먼저 확인되는 반면, DLB 환자군은 Fz 위치에서 P300 반응의 진폭이 우선적으로 관찰되었다. DLB 환자의 P300 반응을 확인한 Kurita 등[19]의 연구에서도 정상 대조군과의 비교에서 N200과 P300 반응의 잠복기에서 DLB 환자의 잠복기 지연으로 인한 유의한 차이가 확인되었다[(N2 잠복기=정상 대조군: 242.2±37.7, DLB: 284.2±52.2, p<0.01), (P3 잠복기=정상 대조군: 378.8±44.7, DLB: 429.5±87.7, p<0.05)]. 결과를 종합해 보면, P300 잠복기는 AD과 DLB 환자에서 모두 지연되는 결과를 보여주어 절대 잠복기는 정상 대조군과 AD, DLB 환자를 구분하는 지표가 될 수 있으며, 반응의 위치에 따른 잠복기 변화로 AD 환자와 DLB 환자를 구분할 수 있다.
Brønnick 등[17]은 여러 유형의 치매 환자군에게 MMN을 적용하여 청각 자극의 선택적 주의력을 확인하였다. 연구 대상자들은 DLB, PDD, PD, AD, 정상 대조군의 총 5그룹으로 구성되었다. 결과를 요약하면 MMN 반응의 진폭은 PD 환자군에서 가장 크게 관찰되었으며(-3.67±1.24), 뒤이어 DLB(-3.34±1.42), 정상 대조군(-3.14±1.05), AD(-2.59±1.78), PDD(-2.31±0.92)순으로 관찰되어, DLB 환자군과 PDD 환자군 간 MMN 반응 진폭에서 유의한 차이가 관찰되었다(p=0.02). MMN 반응 면적 또한 DLB 환자군(-82.43±50.34)과 PDD 환자군(-29.15±66.04) 간 유의한 차이가 확인되어(p=0.017), 진폭과 면적에서 PDD 환자군이 가장 작은 반응을 나타냈다.
주관적 중추청각행동검사
Maeshima 등[27]은 청각 언어 학습 검사를 사용하여 AD, DLB, 혈관성치매(vascular dementia, VD), 전두측두엽치매(frontotemporal dementia, FTD), 노인 대조군 대상자의 청각 단어 회상 능력을 평가하였다. 결과적으로 즉시회상과 지연회상 검사에서 청각 단어 회상 능력은 대조군과 모든 치매환자군간 유의한 차이가 확인되었다[(즉시회상=AD: 13.9±8.2, VD: 16.2±7.1, FTD: 18.6±8.4, DLB: 15.3±7.1, 노인 대조군: 33.4±7.5, p<0.0001), (지연회상=AD: 0.28±0.92, VD: 0.69±1.56, FTD: 0.50±1.15, DLB: 0±0, 노인 대조군: 4.91±3.34, p<0.0001)]. DLB와 PDD 환자를 대상으로 단어인지 검사를 통해 청각 언어 인지 능력을 확인한 Wesnes 등[20]의 선행 연구에서는 Memantine 약의 효과를 확인하기 위하여 위약군과 실험군으로 PDD 환자와 DLB 환자를 무작위로 할당하여 배치하였다. 그러나, 아쉽게도 해당 문헌에서는 PDD와 DLB 환자의 실제적인 각각의 데이터는 확인할 수 없었다.
PDD 환자의 청각 기능을 위한 체계적 연구결과 분석
대상자가 중복된 문헌을 포함하여 PDD 환자군은 6개의 문헌이 확인되었다. 문헌의 수의 부족과 검사 도구의 이질성으로 인해 DLB 환자군에서와 마찬가지로 메타 분석이 불가능하였다. 따라서 체계적 연구결과분석을 실시 후 Table 4에 결과를 요약하였다.
객관적 청각유발전위 검사
Kurita 등[19]은 AD, DLB, 환시의 증상을 보이는 PDD, 환시의 증상이 없는 PDD 환자군을 대상으로 청성후기반응(N100, P200, N200, P300)을 측정하였다. 환시가 없는 PDD 대상자와 정상 대조군과의 P300의 잠복기에서 유의한 차이가 관찰되었으며(정상 대조군: 378.8±44.7, 환시가 없는 PDD: 445.3±66.1, p<0.01), 환시가 있는 PDD 대상자와 정상 대조군의 N200 잠복기(정상 대조군: 242.2±37.7, 환시가 있는 PDD: 283.2±52.3, p<0.05)와 P300 잠복기(정상 대조군: 378.8±44.7, 환시가 있는 PDD: 436.4±89.3, p<0.05)에도 유의한 차이가 관찰되었다. 앞서 확인한 Brønnick 등[17]의 연구에서도 MMN 반응은 DLB 환자군과 PDD 환자군 간에 진폭(p=0.02)과 면적(p=0.017)에서 유의한 차이가 관찰되었다. Yamamoto 등[28]의 연구에서는 PDD 환자의 P300 반응 잠복기와 MMSE 점수의 상관분석을 실시하였고, PDD 대상자의 P300 잠복기 결과는 MMSE 점수가 17 이상인 경증 치매 환자에서 MMSE 점수와 강한 음의 상관 관계를 보여주었다(r=-0.808; p<0.001).
주관적 중추청각행동검사
주관적 측정방법을 활용하여 PDD 환자군의 청각 능력을 확인한 Claus와 Mohr [29]은 이분청취검사를 실시하였다. 연구 대상자는 AD, 헌팅턴병, PDD, PD, 대조군이 포함되었다. 자유회상 검사의 좌측 귀 수행력에서 PDD 환자군 0.28±0.15의 수행력을 보여 정상 대조군(0.39±0.12, p<0.05)과 파킨슨병 대상자(0.41±0.13, p<0.05)와 유의한 차이를 보였으며, 좌측 귀 회상(left ear recall)검사의 좌측 귀 수행력에서 0.40±0.17의 수행력을 보여 정상 대조군(0.60±0.12, p<0.01)과 PD(0.57±0.16, p<0.05)와 유의한 차이를 보였다. 또한, 우측 귀회상(right ear recall) 검사에서 우측 귀 수행력은 0.44±0.23으로 확인되어 정상 대조군과 유의한 차이를 보였으며(0.64±0.11, p<0.01), 좌측 귀 수행력은 0.28±0.15로 PD와 유의한 차이를 보였다(0.41±0.12, p<0.05). Wesnes 등[20]의 연구에서는 단어 인지 검사를 실시하였지만, PDD 환자만의 순수한 결과는 확인할 수 없었으며, Schmitt 등[30]의 연구에서도 PDD 환자군의 청각 언어인지 검사를 실시하였지만, rivastigmine 약물 복용 및 플라시보 효과에 대한 수행력 변화만을 보고하였다.
결 론
본 종설은 치매 유형에 따른 치매 환자들의 청각 기능을 구분하고자 72건의 AD 환자들의 객관적 청성유발전위 및 주관적 중추청각행동검사의 선행 연구 결과를 바탕으로 메타분석을 실시하였고, DLB 환자군과 PDD 환자군을 대상으로 의미 있는 결과를 보고한 각 5편 및 6편의 논문들의 연구 결과를 체계적으로 분석하였다.
먼저, 청성유발전위 반응의 결과를 기반으로 시행한 메타분석 결과는 AD 환자군과 정상 인지를 갖은 노인 대조군과의 비교에서 N200과 P300 잠복기의 유의한 지연이 관찰되었지만[(N200: SMD=1.144, 95% CI=0.475 to 1.813, p<0.001), (P300: SMD=1.220, 95% CI=0.936 to 1.504, p<0.001)], N100과 P200의 잠복기에서는 유의한 차이가 확인되지 않았다[(N100: SMD=0.672, 95% CI=-0.051 to 1.395, p=0.069), (P200: SMD=0.129, 95% CI=-0.131 to 0.389, p=0.331)]. 이러한 분석은 AD 환자군이 N200의 잠복기부터 순차적으로 유의하게 지연되는 결과를 보여 선행 메타 분석 연구의 결과와 일치성을 나타냈다[3,4]. 또한 P300의 진폭 역시 유의하게 감소된 결과를 나타내 Hedges 등[5]의 메타 분석 결과와 일치하였다. 그러나 선행연구에서도 확인된 높은 이질성은 본 연구에서도 유사하게 확인되었다. Howe 등[4]은 P300 잠복기에 영향을 주는 요인으로 환자군의 평균 연령, 자극 간 간격 및 자극 주파수, 기준 전극, 샘플링 주기를 지적하였고, Hedges 등[5]은 메타 회귀분석을 실시하여 P300 진폭의 결과의 이질성의 원인이 환자군의 교육 수준에 있다고 결론내렸다. 따라서 검사방법, MMSE 점수, 자극의 타입(click/tone), 자극기간, 자극강도, 자극빈도, 평균연령, 교육수준, 기준전극, 자극 주파수, 샘플링주기, 필터 등 다양한 원인들에 의해 청성유발전위의 메타 분석 결과에서 높은 이질성을 보인 것으로 사료되기에 향후 청성유발전위의 검사 셋팅 및 임상적 기준을 보다 명확히 설정하여 일관된 반응을 이끄는 연구들이 필요하다.
주관적 중추청각행동검사에서는 중추청각처리능력, 숫자 바로 따라하기, 숫자 거꾸로 따라하기, 청각 단어 회상 능력에서 유의한 차이가 확인되었다. 또한 중추청각처리검사의 결과가 낮은 이질성과 유의한 수행력의 차이를 보여 임상적 활용 가능성이 높게 판단되었다. 병리학적 위치와 청각적 기능의 연관성을 확인할 때, 대부분은 중추청각처리 과정과 관련이 있음에도 불구하고 중추청각처리능력을 진단할 수 있는 국내의 표준화된 검사가 현재 부재하고 국외에서도 중추청각 처리검사 결과에서 피험자간/피험자내 변이(inter/intra subject variance)가 높기에 실제 임상적 활용은 크지 않다. 그러나 메타 분석에서 의미 있는 결과가 확인된 만큼 향후 치매 환자들을 위한 중추청각처리검사의 적용이 여러 연구에서 시도되어야 하겠다.
한편, DLB 환자와 PDD 환자에게 청각 검사를 적용한 연구들을 체계적으로 결과 분석 시, P300의 잠복기는 DLB와 PDD 환자군 모두 유의하게 지연된 결과를 확인하였고, P300의 진폭 분포 변화는 DLB 환자와 AD 환자, 대조군에서 유의한 차이를 보였다. 또한, PDD 환자군과 DLB 환자군 간에 MMN 진폭 및 면적에서 유의한 차이를 보였다. DLB 환자군은 대조군과의 비교에서 청각 단어 회상 능력의 유의한 차이를 보였으며, PDD 환자군은 이분청취검사에서 우측 귀 수행력이 대조군보다 낮게 나타나 유의한 차이를 보였다.
Table 5는 본 종설 논문에서 다룬 결과들을 종합하여 AD, DLB, PDD 환자군에서 청각 기능의 저하로 확인된 검사들을 표기하였다. DLB와 PDD환자들의 청각적 연구가 매우 적어 본 결과를 일반화하기에는 아직 시기적으로 이르지만, P300 잠복기는 치매의 유형에 상관없이 대조군과 비교 시 모두 유의하게 지연되었다. 따라서 치매의 유무를 확인하기 위한 검사로는 P300 잠복기의 비교를 제안한다. 몇몇 연구에서는 지연된 P300 잠복기의 정도를 통해 치매 유형을 구분하였지만[18], 일부 문헌에서는 지연된 P300 잠복기의 정도가 치매 유형간 유의한 차이를 보이지 않았다[19]. 만약 치매의 유형에 따른 청각 기능의 차이를 구분하고자 한다면, MMN 결과와 P300 진폭 분포 변화를 활용하는 것을 제안한다. 특히 MMN 검사에서는 정상 인지의 대조군과는 통계적 차이가 없었지만, DLB 환자군과 PDD 환자군 간의 비교에서는 유의한 차이를 보여주어 MMN의 진폭 및 면적을 비교하여 치매의 유형 간 차별성을 이끌 수 있을 것으로 사료된다[17].
본 종설의 한계점으로는 아쉽게도 메타 분석 결과에서 높은 이질성이 확인되어 직접적인 임상적 적용은 단언하기 보다는 청성유발전위 검사의 셋팅과 기준에서 클리닉 간 통일성이 필요할 것으로 판단된다. 또한 AD 환자들에 비하여 DLB 및 PDD 환자들을 대상으로 청각적 수행력을 확인한 문헌은 매우 제한적이었다. 따라서 유형별 치매 환자군에게 청각 검사를 적용하고 더 많은 기초 데이터가 축적되어 치매 유형 간 차별화된 청각 선별 도구가 확보될 필요가 있다.