žĄú Ž°†
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖ(solitary fibrous tumor, SFT)žĚÄ ž£ľŽ°ú ŪĚČŽßČžĚė ÍįĄžóĹžĄłŪŹ¨žóźžĄú ÍłįžõźŪēėŽäĒ ŽďúŽ¨ł žĖĎžĄĪ Žį©ž∂ĒžĄłŪŹ¨ žĘÖžĖĎžúľŽ°ú(mesenchymal tumor) 1931ŽÖĄ KlempereržôÄ Rabin [1]žĚī ž≤ėžĚĆžúľŽ°ú Ž≥īÍ≥†ŪēėžėÄŽč§.
ŪĚČŽßČ žôłžóźŽŹĄ Ž≥ĶÍįē, žĘÖÍ≤©ŽŹô, ŪŹź, ÍįĄ, žč†žě• ŽďĪ žč†ž≤ī ž†ĄŽįėžóźžĄú ŽįúžÉĚŪē† žąė žěąžúľŽ©į[2], ŽĎźÍ≤ĹŽ∂Ä žėĀžó≠žóźžĄúŽäĒ ÍĶ¨Íįē, ŽĻĄÍįē, Žąą, ŪõĄŽĎź, ÍįĎžÉĀžĄ†, žĻ®žÉė, Ž∂Ğ̳ŽĎźÍįē ŽďĪžóźžĄú ŽįúžÉĚŪēúŽč§[3]. žĚīž§Ď žôłžĚīŽŹĄžóźžĄú ŽįúžÉĚŪēėŽäĒ Í≤ĹžöįŽäĒ ÍĶ≠žôł 4žėą, ÍĶ≠Žāī 1žėąŽ°ú Žß§žöį ŽďúŽ¨ľÍ≤Ć Ž≥īÍ≥†ŽźėžóąŽč§(Table 1).
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ ž°įžßĀŪēôž†Ā Í≤Äžā¨Ž•ľ ŪÜĶŪēī žßĄŽč®ŪēėŽ©į, žĚīžóź ÍįźŽ≥ĄŪēīžēľ Ūē† žßąŪôėžúľŽ°úŽäĒ žč†Í≤ĹžĄ¨žú†žĘÖ, žč†Í≤ĹžīąžĘÖ, žĄ¨žú†žú°žĘÖ, ŪėąÍīÄž£ľžúĄžĄłŪŹ¨žĘÖ ŽďĪžĚī žěąŽč§[4]. ŪėĄžě¨ÍĻĆžßÄ žôłžĚīŽŹĄžóźžĄú ŽįúžÉĚŪēú Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ Žß§žöį ŽďúŽ¨ľžĖī Í∑ł ŪäĻžĄĪžĚĄ ŽÖľžĚėŪēėÍłī žĖīŽ†§žöįŽāė, ŪĚČŽßČ žôł Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚė ŪäĻžĄĪžĚĄ Í≥†Ž†§ŪēīŽ≥łŽč§Ž©ī žēÖžĄĪ ŽįŹ žě¨Žįú ÍįÄŽä•žĄĪžĚī žěąžúľŽĮÄŽ°ú[5], ÍįÄŽä•ŪēėŽ©ī žąėžą†ž†ĀžúľŽ°ú žôĄž†ĄŪěą ž†ąž†úŽźėžĖīžēľ ŪēúŽč§[4].
Ž≥ł ž†ÄžěźŽď§žĚÄ 55žĄł Žā®ŪôėžĚė žôłžĚīŽŹĄžóź ŽįúžÉĚŪēú Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖ 1žėąŽ•ľ Í≤ĹŪóėŪēėžėÄÍłįžóź žĚīŽ•ľ Ž¨łŪóĆ Í≥†žįįÍ≥ľ Ūē®ÍĽė Ž≥īÍ≥†ŪēėÍ≥†žěź ŪēúŽč§.
ž¶Ě Ž°Ä
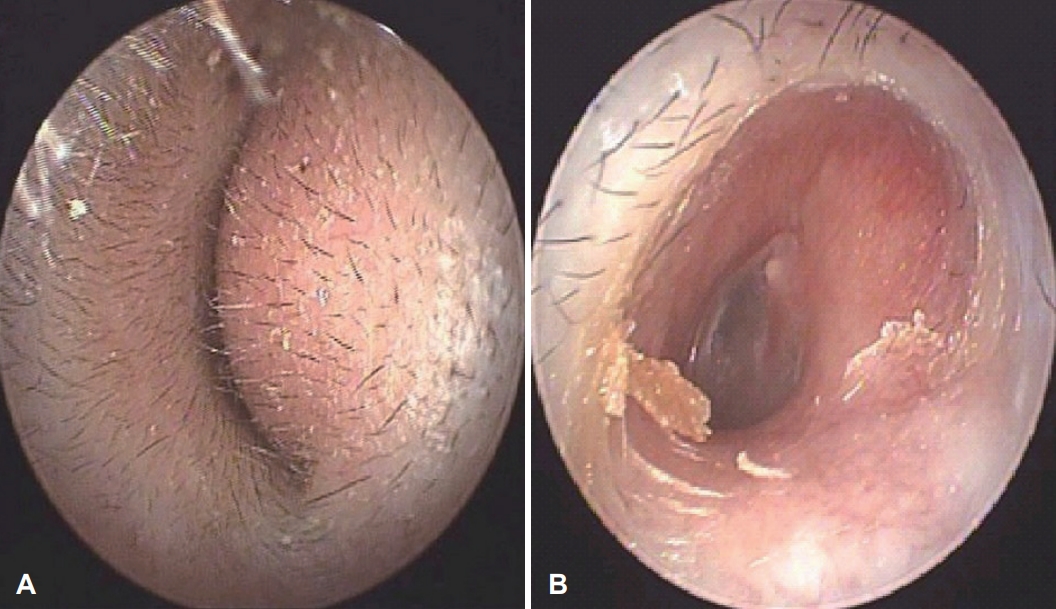
55žĄł Žā®žěź ŪôėžěźÍįÄ žöįžóįŪěą ŽįúÍ≤¨Žźú žĘĆžł° žôłžĚīŽŹĄžĚė žĘÖŽ¨ľžĚĄ ž£ľžÜĆŽ°ú ŽāīžõźŪēėžėÄŽč§. ŪôėžěźŽäĒ Ž¨łžßĄžóźžĄú žĚīž∂©ŽßĆÍįźžĚĄ ŪėłžÜĆŪēėžėÄÍ≥†, Žāúž≤≠, žĚīŽ™Ö, žĚīŪÜĶ, žĖīžßÄŽüľž¶Ě ŽďĪžĚė Žč§Ž•ł žĚīÍ≥ľž†Ā ž¶ĚžÉĀžĚÄ ŪėłžÜĆŪēėžßÄ žēäžēėŽč§. Í≥ľÍĪįŽ†•žÉĀ Í≥†Ūėąžēē žôłžóź ÍįÄž°ĪŽ†• ŽįŹ žā¨ŪöĆŽ†•žÉĀ ŪäĻžĚīžā¨Ūē≠žĚÄ žóÜžóąŽč§. žĚīŪēôž†Ā Í≤Äžā¨žÉĀ žĘĆžł° žôłžĚīŽŹĄŽ•ľ žôĄž†ĄŪěą Ž©ĒžöįŽäĒ žĘÖŽ¨ľžĚī žôłžĚīŽŹĄ žěÖÍĶ¨žĚė ŪõĄŽ≤Ş󟞥ú ÍīÄžįįŽźėžóąžúľŽ©į, žĘÖŽ¨ľžĚÄ ŽĻĄÍĶźž†Ā Žč®Žč®ŪēėžėÄÍ≥†, Í≤ĹÍ≥ĄÍįÄ Ž∂ĄŽ™ÖŪēėžėÄŽč§(Fig. 1A). Í≥†ŽßČžĚÄ žĘÖŽ¨ľŽ°ú žĚłŪēėžó¨ ŪôēžĚłžĚī žĖīŽ†§žõ†Í≥†, žąúžĚĆž≤≠Ž†•Í≤Äžā¨žóźžĄú 6Ž∂ĄŽ≤ēžÉĀ žöįžł°žĚÄ 10 dB HL, žĘĆžł°žĚÄ 17 dB HL, žĖīžĚĆŽ≥ÄŽ≥ĄŽ†•Í≤Äžā¨žÉĀ žöįžł°žĚÄ 100%, žĘĆžł°žĚÄ 92% ŪôēžĚłŽźėžóąŽč§.
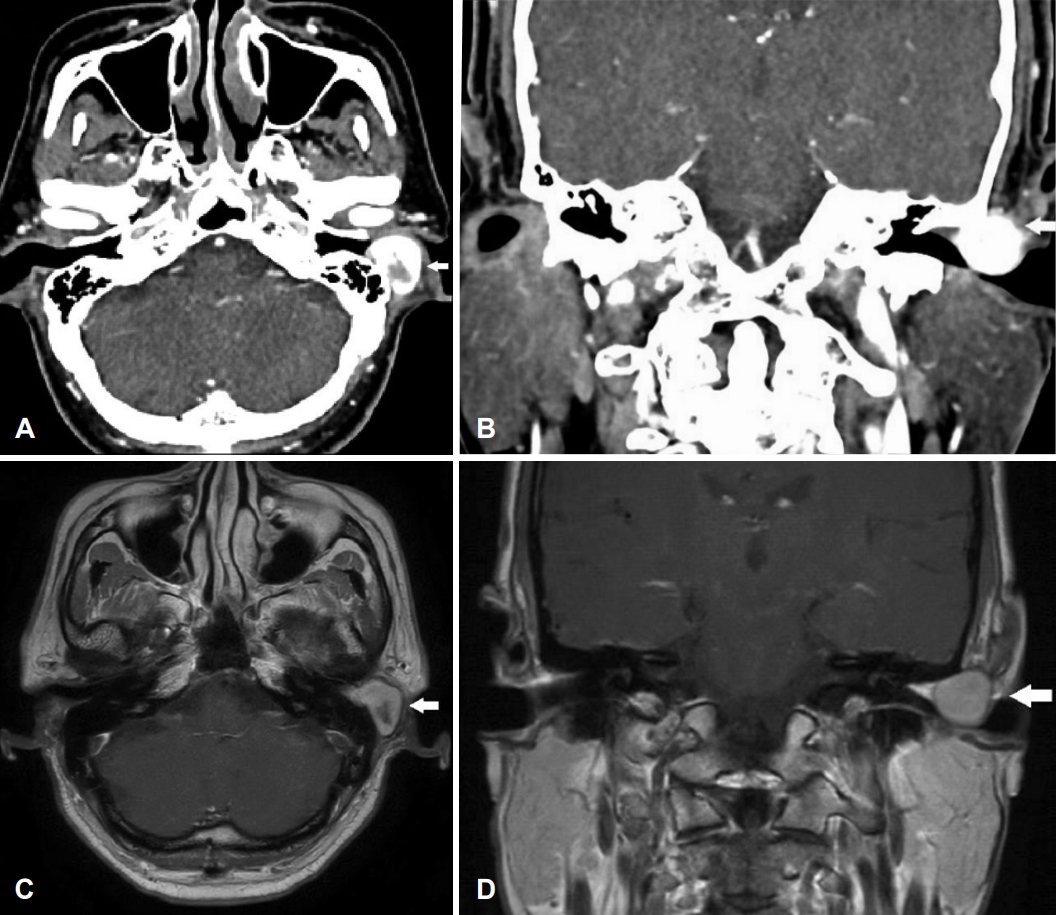
ž†ĄžāįŪôĒŽč®žłĶžī¨žėĀ žėĀžÉĀžóźžĄú ž°įžėĀž†ú Ūą¨žó¨žčú Ž∂ąÍ∑†žĚľŪēėÍ≤Ć ž°įžėĀ ž¶ĚÍįēžĚĄ Ž≥īžĚīŽ©į, Í≤ĹÍ≥ĄÍįÄ Ž∂ĄŽ™ÖŪēú 2.0√ó1.7 cm ŪĀ¨ÍłįžĚė žĘÖŽ¨ľžĚī žĘĆžł° žôłžĚīŽŹĄžóź žúĄžĻėŪēėÍ≥† žěąžóąÍ≥†, žôłžĚīŽŹĄÍįÄ Žß§žöį žĘĀžēĄžßĄ žÜĆÍ≤¨žĚīžóąŽč§(Fig. 2A and B). žěźÍłįÍ≥ĶŽ™ÖžėĀžÉĀžóźžĄúŽŹĄ žĘĆžł° žôłžĚīŽŹĄžóź žĘÖŽ¨ľžĚī ŪôēžĚł ŽźėžóąÍ≥†, ž°įžėĀž†ú Ūą¨žó¨žčú Ž∂ąÍ∑†žĚľŪēú ž°įžėĀ ž¶ĚÍįēžĚĄ Ž≥īžėÄŽč§. ŽėźŪēú ž£ľŽ≥Ä ž°įžßĀžúľŽ°úžĚė žĻ®Ž≤ĒžĚīŽāė Ž≥ÄŪėēžĚÄ Ž≥īžĚīžßÄ žēäžēėŽč§(Fig. 2C and D). žīąžĚĆŪĆĆ žú†ŽŹĄŪēė žĄłžĻ®ŪĚ°žĚłÍ≤Äžā¨Ž•ľ žčúŪĖČŪēėžėÄÍ≥†, žĘÖŽ¨ľžóźžĄú ŽĻĄž†ĄŪėēž†ĀžĚł žĄłŪŹ¨ŽäĒ Ž≥īžĚīžßÄ žēäžēėžúľŽ©į, žĄ¨žú† ž°įžßĀ(fibrous tissue)žĚī ŪôēžĚłŽźėžóąŽč§.
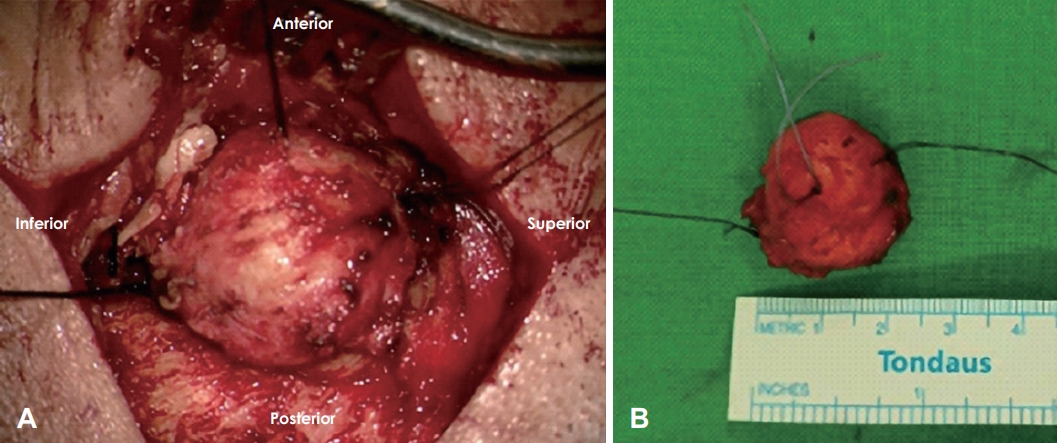
ž†Ąžč† Žßąž∑®Ūēė ŽĮłžĄłžąėžą† ŪėĄŽĮłÍ≤Ş̥ žĚīžö©Ūēėžó¨ ŪõĄžĚīÍįú ž†ĎÍ∑ľŽ≤ēžúľŽ°ú žĘÖŽ¨ľžĚĄ ž†ąž†úŪēėžėÄŽč§(Fig. 3A). žú°žēą žÜĆÍ≤¨žÉĀ 2.3√ó2√ó1.5 cm ŪĀ¨ÍłįžĚė Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēú žóįž°įžßĀ žĘÖŽ¨ľžĚī ŪôēžĚłŽźėžóąŽč§(Fig. 3B). žąėžą†ž†Ā žôĄž†Ą ž†ąž†ú ŪõĄ Í∑Ä ŪĆ®ŪāĻžĚĄ žčúŪĖČŪēėžėÄŽč§. ŪôėžěźŽäĒ žąėžą† ŪõĄ 1žĚľžßł, ŪäĻŽ≥ĄŪēú Ūē©Ž≥Ďž¶Ě žóÜžĚī ŪáīžõźŪēėžėÄŽč§.
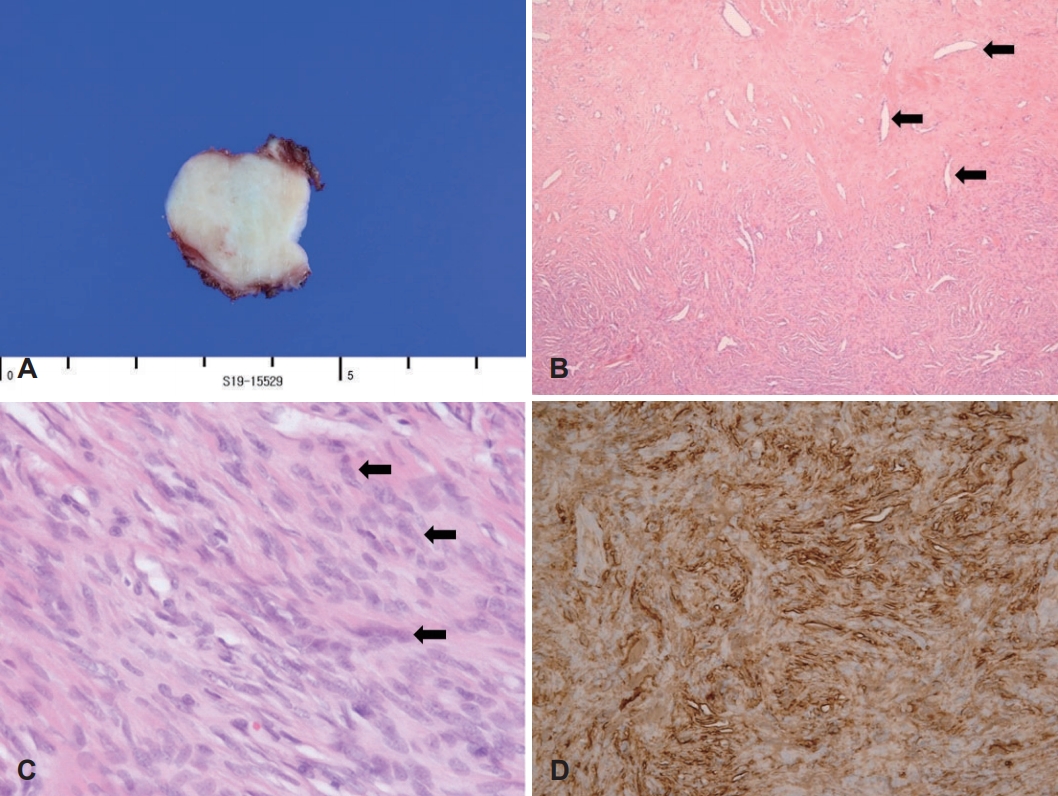
Ž≥ĎŽ¶¨ž°įžßĀÍ≤Äžā¨žÉĀ ž†Ąž≤ī Í≤Äž≤īžĚė Žč®Ž©īžĚÄ ŪöĆŽįĪžÉČžúľŽ°ú Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēėžėÄÍ≥†(Fig. 4A), Žį©ž∂ĒžĄłŪŹ¨(spindle cell)ÍįÄ ŽßéžĚÄ žßÄžó≠Í≥ľ žĄłŪŹ¨ÍįÄ ž†ĀÍ≥† žĄ¨žú†žßąŽ°ú žĪĄžõƞߥ žßÄžó≠Žď§žĚī Ž∂ąÍ∑úžĻôŪēú ŪėēŪÉúŽ°ú ŽāėŪÉÄŽā¨žúľŽ©į, žā¨žäīŽŅĒ Ž™®žĖĎžĚė ŪėąÍīĎ吏Ěī Ūē®ÍĽė ÍīÄžįįŽźėžóąŽč§(Fig. 4B). ŽėźŪēú Žč®ž°įŽ°úžöī ŪēĶžĚĄ ÍįĞߥ žĄ¨žú†žēĄžĄłŪŹ¨žôÄ ÍĶźžõźžĄĪÍłįžßąžĚī Ūėľžě¨Žźú žĖĎžÉĀžĚĄ Ž≥īžėÄÍ≥†(Fig. 4C), Ž©īžó≠ž°įžßĀŪôĒŪēôžóľžÉČ(immunohistochemical stain)žóźžĄú CD34žóź žĖĎžĄĪ ŽįėžĚϞ̥ ŽāėŪÉÄŽāīžĖī(Fig. 4D), Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžúľŽ°ú žßĄŽč®ŪēėžėÄŽč§. ŪôėžěźŽäĒ žąėžą† ŪõĄ 9ÍįúžõĒ ŽŹôžēą žě¨Žįú žÜĆÍ≤¨ žóÜžĚī Í≤ĹÍ≥ľ ÍīÄžįį ž§ĎžĚīŽč§(Fig. 1B).
Í≥† žįį
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖ(SFT)žĚÄ ŽĆÄŽ∂ÄŽ∂Ą ž§ĎŽÖĄžóźžĄú ž£ľŽ°ú ŽįúžÉĚŪēėŽ©į, Žā®ŽÖÄ žú†Ž≥ĎŽ•†žĚÄ ŽĻĄžä∑ŪēėŽč§[5]. ŽĆÄŽ∂ÄŽ∂ĄžĚė Í≤Ĺžöį ž¶ĚžÉĀžĚÄ žóÜžúľŽāė ŽįúžÉĚŽźėŽäĒ žúĄžĻėŽāė ŪĀ¨Íłįžóź ŽĒįŽĚľ ÍĶ≠žÜĆž†Ā ž¶ĚžÉĀžĚĄ Ž≥īžĚīŽäĒ Í≤ĹžöįŽŹĄ žěąŽč§[3].
žĚīž†úÍĻĆžßÄ Ž≥īÍ≥†Žźú ž¶ĚŽ°ÄžóźžĄú, žôłžĚīŽŹĄžóźžĄú ŽįúžÉĚŪēú Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖ ŪôėžěźžĚė ŽĆÄŽ∂ÄŽ∂ĄžĚÄ žôłžĚīŽŹĄ ŪŹźžáĄŽ°ú žĚłŪēú ž≤≠Ž†•ÍįźžÜĆŽ•ľ ž£ľŽ°ú ŪėłžÜĆ ŪēėžėÄžúľŽ©į, ž¶ĚžÉĀžĚī žóÜŽäĒ Í≤ĹžöįŽŹĄ žěąžóąŽč§(Table 1). Ž≥ł ž¶ĚŽ°ÄžóźžĄú ŪôėžěźŽäĒ žĘĆžł° žĚīž∂©ŽßĆÍįźžúľŽ°ú ŽāīžõźŪēėžėÄžúľŽ©į, ž≤≠Ž†•ÍįźžÜĆŽ•ľ ŪėłžÜĆŪēėžßÄŽäĒ žēäžēėŽč§. žąúžĚĆž≤≠Ž†•Í≤Äžā¨žÉĀ žĘĆžł° 17 dBŽ°ú žöįžł° 10 dBžóź ŽĻĄŪēī Í≥†ž£ľŪĆĆ žėĀžó≠žóźžĄú ž≤≠Ž†• žó≠žĻėžĚė žÉĀžäĻ žÜĆÍ≤¨žĚī Ž≥īžĚīŽāė, žĚīŽäĒ žĘÖŽ¨ľŽ°ú žĚłŪēú ÍįÄŽä•žĄĪžĚÄ ŽĖ®žĖīžßÄŽäĒ Í≤ÉžúľŽ°ú žÉĚÍįĀŽźúŽč§.
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ Žč§Ž•ł žóįž°įžßĀ žĘÖžĖĎÍ≥ľ žėĀžÉĀŪēôž†Ā Í≤Äžā¨ Í≤įÍ≥ľÍįÄ žú†žā¨Ūēėžó¨ žßĄŽč®žĚĄ žúĄŪēú ŪäĻžßēž†ĀžĚł žÜĆÍ≤¨žĚÄ žóÜŽč§. ž†ĄžāįŪôĒŽč®žłĶžī¨žėĀ žėĀžÉĀžóźžĄúŽäĒ ž†ÄžĚĆžėĀ žĘÖŽ¨ľŽ°ú Ž≥īžĚīÍ≥†, ž°įžėĀž†ú Ūą¨žó¨žčú Ž∂ąÍ∑†žĚľŪēėÍ≤Ć ž°įžėĀ ž¶ĚÍįēžĚĄ Ž≥īžĚīŽ©į, žĘÖŽ¨ľžĚė žēēŽ†•žúľŽ°ú žĚłŪēú Í≥®ŪĆĆÍīīžĚė žÜĆÍ≤¨žĚī ŽŹôŽįėŽźėÍłįŽŹĄ ŪēúŽč§[1]. ŽėźŪēú, žěźÍłįÍ≥ĶŽ™ÖžėĀžÉĀžĚė T1-Íįēž°įžėĀžÉĀžóźžĄúŽäĒ Í≤ĹÍ≥ĄÍįÄ ŽöúŽ†∑Ūēú žĘÖŽ¨ľžĚī Í∑ľžú°Í≥ľ ŽŹôŽďĪŪēú žč†ŪėłÍįēŽŹĄŽ°ú ŽāėŪÉÄŽāėÍĪįŽāė ž†ÄÍįēŽŹĄ žč†ŪėłŽ°ú ŽāėŪÉÄŽāėŽ©į, T2-Íįēž°įžėĀžÉĀžóźžĄú ž†Äžč†ŪėłÍįēŽŹĄ ŽįŹ Í≥†žč†ŪėłÍįēŽŹĄÍįÄ Ž∂ąÍ∑úžĻôŪēėÍ≤Ć ŽāėŪÉÄŽāėÍ≥†, ž°įžėĀž†ú Ūą¨žó¨žčú Ž∂ąÍ∑†žĚľŪēú ž°įžėĀ ž¶ĚÍįēžĚĄ Ž≥īžĚłŽč§[10].
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚė ž°įžßĀŪēôž†Ā žÜĆÍ≤¨žĚÄ žßĄŽč®žóź žěąžĖīžĄú ž§ĎžöĒŪēėŽč§. ŪėĄŽĮłÍ≤Ĺ Í≤Äžā¨žÉĀ žĘÖŽ¨ľžĚė Í≤ĹÍ≥ĄÍįÄ Ž™ÖŪôēŪēėÍ≥†, Žį©ž∂ĒŪėē žĄłŪŹ¨žôÄ ÍĶźžõźžßąžĚī Ž∂ąÍ∑úžĻôŪēėÍ≤Ć ŽįįžóīŽźú ŪäĻžßēžĚī žěąŽč§[4]. Ž©īžó≠ž°įžßĀŪôĒŪēôžóľžÉȞ󟞥ú ŪäĻžßēž†ĀžúľŽ°ú CD34 Ūē≠žõźžóź žĖĎžĄĪŽįėžĚϞ̥ Ž≥īžĚīŽ©į, Í∑ł žôłžóźŽŹĄ vimentin, bcl-2 ŽďĪžóź žĖĎžĄĪŽįėžĚϞ̥ Ž≥īžĚīÍ≥†, cytokeratine, S-100 protein, desmin, muscle-specific actin, smooth-muscle actinžóźŽäĒ ŽĆÄŽ∂ÄŽ∂Ą žĚĆžĄĪŽįėžĚϞ̥ Ž≥īžĚłŽč§[4]. žĚī žóľžÉČ Žį©Ž≤ēžĚĄ ŪÜĶŪēī Žį©ž∂ĒžĄłŪŹ¨Ž•ľ ÍįÄžßÄŽäĒ Žč§Ž•ł žóįŽ∂Ä ž°įžßĀ žĘÖžĖĎÍ≥ľ ÍįźŽ≥ĄŪē† žąė žěąÍ≥†, žĚīžóź ÍįźŽ≥ĄŪēīžēľ Ūē† žßąŪôėžúľŽ°ú žč†Í≤ĹžĄ¨žú†žĘÖ, žč†Í≤ĹžīąžĘÖ, žĄ¨žú†žú°žĘÖ, ŪėąÍīÄž£ľžúĄžĄłŪŹ¨žĘÖ ŽďĪžĚī žěąŽč§[4]. Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ Ž©īžó≠ž°įžßĀŪôĒŪēôžóľžÉČ(immunohistochemical stain)žóźžĄú CD34žóź žĖĎžĄĪ, S-100 protein žĚĆžĄĪ, C-kit žĚĆžĄĪ, desmin žĚĆžĄĪ, actin žĚĆžĄĪ, EMA žĚĆžĄĪžúľŽ°ú ŽāėŪÉÄŽāīžĖī Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžúľŽ°ú žßĄŽč®ŪēėžėÄŽč§.
Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ ŽĆÄŽ∂ÄŽ∂Ą žĖĎžĄĪžĚīŽāė, ŽďúŽ¨ľÍ≤Ć žēÖžĄĪžĚī ŽįúžÉĚŪēėŽäĒ Í≤ĹžöįŽŹĄ žěąŽč§[11]. ChanžĚÄ ž°įžßĀ žÜĆÍ≤¨žÉĀ ŽÜížĚÄ žĄłŪŹ¨ž∂©žč§žĄĪ(celluarity), žĄłŪŹ¨Žč§ŪėēžĄĪ(pleomorphism), ŽÜížĚÄ žú†žā¨Ž∂ĄžóīŽ•†(10 high power fieldžóźžĄú 4Íįú žĚīžÉĀžĚė žú†žā¨Ž∂Ąžóī)žĚī Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚė žēÖžĄĪŪôĒ ÍįÄŽä•žĄĪžĚĄ ŽāėŪÉÄŽāłŽč§Í≥† ŪēėžėÄŽč§[11]. ŽėźŪēú ž°įžßĀ žÜĆÍ≤¨žÉĀ žĻ®žú§žĄĪ Í≤ĹÍ≥Ą, Íīīžā¨, ž∂úŪėąŽŹĄ žēÖžĄĪžĚė ÍįÄŽä•žĄĪžĚĄ ŽāėŪÉÄŽāłŽč§[2]. žĚīŽü¨Ūēú Íłįž§ÄžúľŽ°ú Ž≥ľ ŽēĆ, Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ žĄłŪŹ¨ ŽįÄŽŹĄÍįÄ ŽāģžēėÍ≥†, žú†žā¨Ž∂ĄžóīžąėŽäĒ 10 high power fieldžóźžĄú 0~1ÍįúžėÄžúľŽ©į, Í≤ĹÍ≥ĄÍįÄ ŽöúŽ†∑ŪēėÍ≥† ž∂úŪėą ŽįŹ Íīīžā¨žĚė žÜĆÍ≤¨žĚī žóÜžĖī žēÖžĄĪžĚė ÍįÄŽä•žĄĪžĚÄ ŽāģžĚĄ Í≤ÉžĚīŽĚľÍ≥† ŪĆźŽč®ŪēėžėÄŽč§.
žĻėŽ£ĆŽäĒ žĘÖŽ¨ľžĚĄ žąėžą†ž†ĀžúľŽ°ú žôĄž†ĄŪěą ž†ąž†úŪēėŽäĒ Í≤ÉžĚīŽč§. Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ žēÖžĄĪ ŽįŹ žě¨ŽįúžĚė ÍįÄŽä•žĄĪžĚī žěąžúľŽĮÄŽ°ú[5], ÍįÄŽä•ŪēėŽ©ī žąėžą†ž†ĀžúľŽ°ú žôĄž†ĄŪěą ž†ąž†úŽ•ľ Ūēīžēľ ŪēúŽč§[4]. ŽėźŪēú žĘÖžĖĎžĚė ŪĀ¨ÍłįÍįÄ 5 cm žĚīžÉĀžĚīÍĪįŽāė Ž∂ąžôĄž†ĄŪēėÍ≤Ć ž†ąž†úŽźú Í≤Ĺžöį, ŪėąÍīÄžĚīŽāė žč†Í≤Ĺ žĻ®Ž≤Ē žÜĆÍ≤¨žĚī žěąŽäĒ Í≤ĹžöįžóźŽäĒ ŪäĻŪěą žēÖžĄĪ ŽįŹ žě¨ŽįúžĚė ÍįÄŽä•žĄĪžĚī ŽÜížúľŽĮÄŽ°ú, žąėžą† ŪõĄ Žį©žā¨žĄ† žĻėŽ£ĆŽ•ľ Í≥†Ž†§Ūēīžēľ ŪēúŽč§[12].
Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ žĘÖŽ¨ľžĚė žąėžą†ž†Ā žôĄž†Ą ž†ąž†ú žĚīŪõĄ ž∂ĒÍįÄž†ĀžĚł ž≤ėžĻėŽ•ľ žčúŪĖČŪēėžßÄ žēäžēėŽč§. 9ÍįúžõĒÍįĄ žě¨Žįú žÜĆÍ≤¨ žóÜžĚī Í≤ĹÍ≥ľ ÍīÄžįį ž§ĎžĚīŽ©į, žě¨ŽįúžĚė ÍįÄŽä•žĄĪžĚī žěąžúľŽĮÄŽ°ú žßÄžÜ枆ĀžúľŽ°ú ž∂Ēž†Ā ÍīÄžįį ž§ĎžĚīŽč§. Í≥†Ž¶ĹžĄĪ žĄ¨žú†žĘÖžĚÄ žôłžĚīŽŹĄžóźžĄú Žß§žöį ŽďúŽ¨ľÍ≤Ć ŽįúžÉĚŪēėŽĮÄŽ°ú žēěžúľŽ°ú ž∂ĒÍįÄž†ĀžĚł ž¶ĚŽ°Ä ŽįúŪĎúžôÄ žóįÍĶ¨ÍįÄ žĚīŽ£®žĖīž†łžēľ Ūē† Í≤ÉžĚīŽ©į, žĚīŽ•ľ ŪÜĶŪēī ž°įÍłįžóź žßĄŽč®Í≥ľ žĻėŽ£ĆÍįÄ žĚīŽ£®žĖīžßą žąė žěąžĚĄ Í≤ÉžĚīŽč§. žĶúÍ∑ľ ž†ÄžěźŽď§žĚÄ žĚīŽ•ľ žĻėŽ£ĆŪēú Í≤ĹŪóėžĚĄ Ž¨łŪóĆ Í≥†žįįÍ≥ľ Ūē®ÍĽė Ž≥īÍ≥†ŪēėŽäĒ ŽįĒžĚīŽč§.