Introduction
Cholesterol granulomas can occur anywhere in the body, with the most common site being the temporal bone [1]. Cholesterol granulomas are often associated with otitis media and are characterized by a blue tympanic membrane on otoscopic examination [2]. Cholesterol granulomas frequently invade the middle ear or petrous apex and can lead to hearing impairments [2];) however, a cholesterol granuloma that extensively destroys the bone structure and invades the cranium is uncommon [1], and cholesterol granuloma cases extending from the mastoid cavity to the cranial cavity without lesions in the middle ear or petrous apex are rarely discussed in the literature. We report on a case of a temporal bone mass extending into the cranial cavity that was found incidentally without accompanying otologic signs or symptoms and was confirmed as a cholesterol granuloma postoperatively.
Case
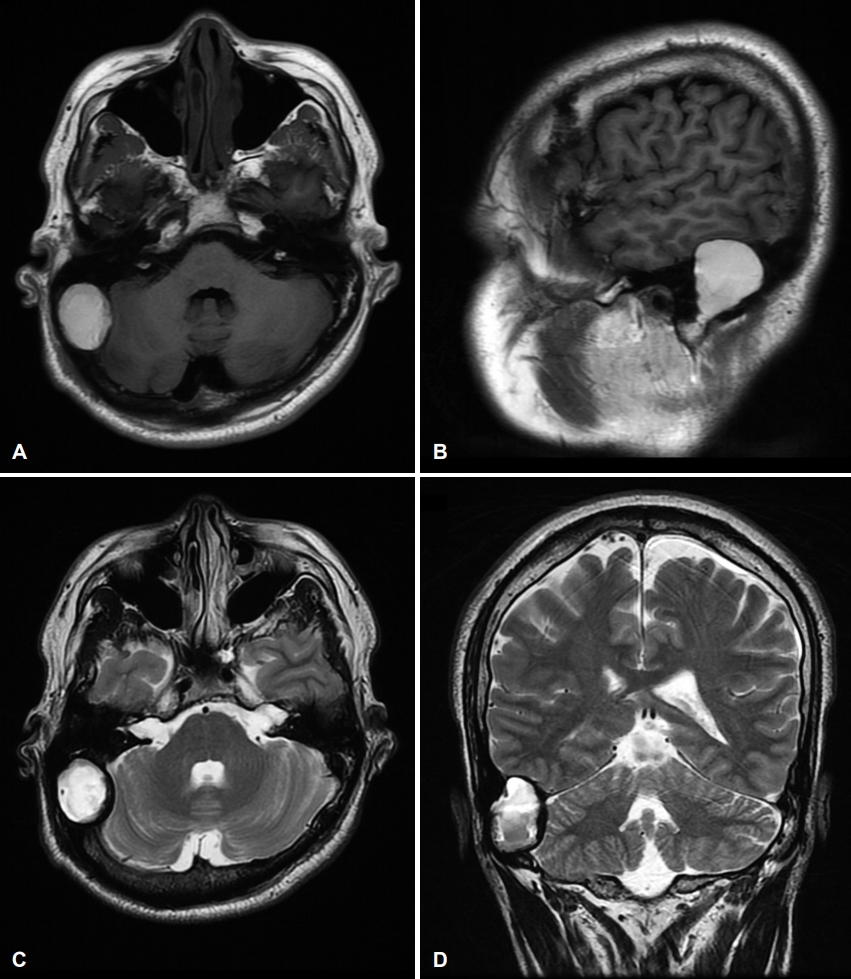
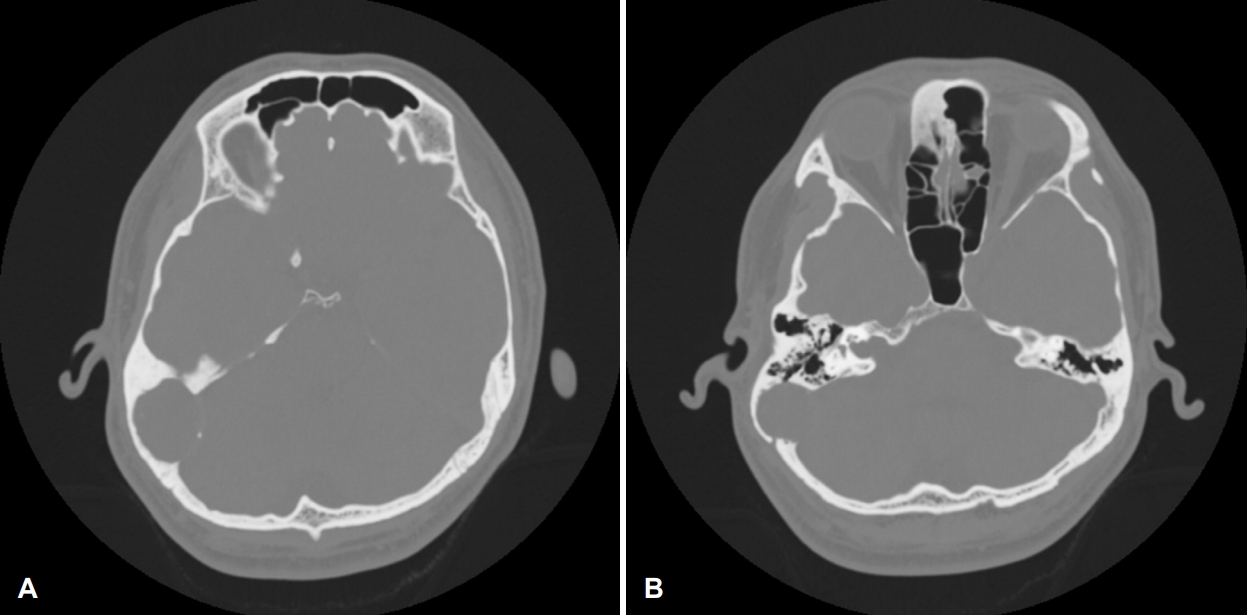
A 31-year-old male visited our clinic, presenting with a suspicious mass lesion in the right temporal bone that had been found incidentally on a brain MRI during a routine health checkup. The patient reported being in a traffic accident three months before, but there was no serious head trauma and no other relevant medical history. On physical examination, both eardrums were intact, and no otologic symptoms such as hearing loss, tinnitus, otalgia, or otorrhea were observed. Brain MRI imaging revealed a 3.5 cm soft tissue mass extending from the right mastoid process to the posterior cranial fossa. The mass demonstrated high signal intensity on T1-weighted images and high signal intensity mixed with partial iso-signal intensity on T2-weighted images. The mass was confined to the epidural space, and no evidence of brain parenchymal infiltration was observed (Fig. 1). A brain CT scan revealed a non-enhancing mass lesion with focal calcification at the posterior fossa, with expansion and remodeling of the outer table, erosion of the inner table, focal bony defect with a thin wall in mastoid air cell, and compression of the sigmoid sinus to the medial side (Fig. 2).
We performed a mass excision via transmastoid and suboccipital craniotomy in cooperation with the neurosurgery department. A simple mastoidectomy was done and there was no abnormality in the mastoid air cells. Only the outer part of the skull bone remained, and the inner part was defective. Through the skull defect, the dura mater of the middle cranial fossa and posterior cranial fossa was exposed (Fig. 3A). The cyst wall was thick and very tightly adherent to the underlying dura mater and sigmoid sinus. The cyst was filled with brown colored cystic fluid along with semisolid components including a glistening material (Fig. 3B). The cystic and semisolid components in the cyst were evacuated. No evidence of involvement of the lesion in the middle ear or brain parenchyma was observed. A small tearing occurred in the transverse sinus during cyst wall dissection but was corrected uneventfully. The defect in the extradural area was filled with abdominal fat, and the craniotomy site was reconstructed using a temporal bone outer table bony fragment and miniplate (Fig. 3C).
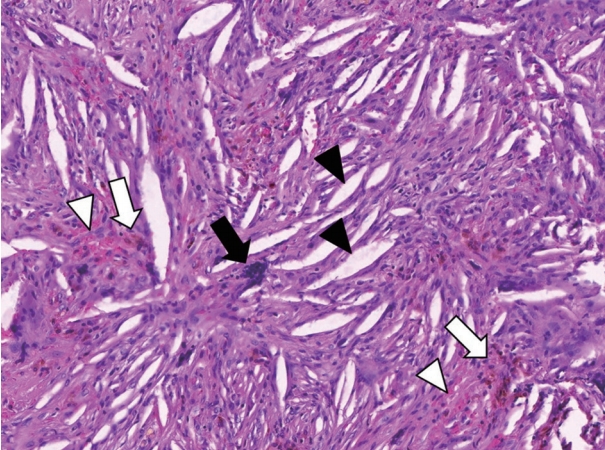
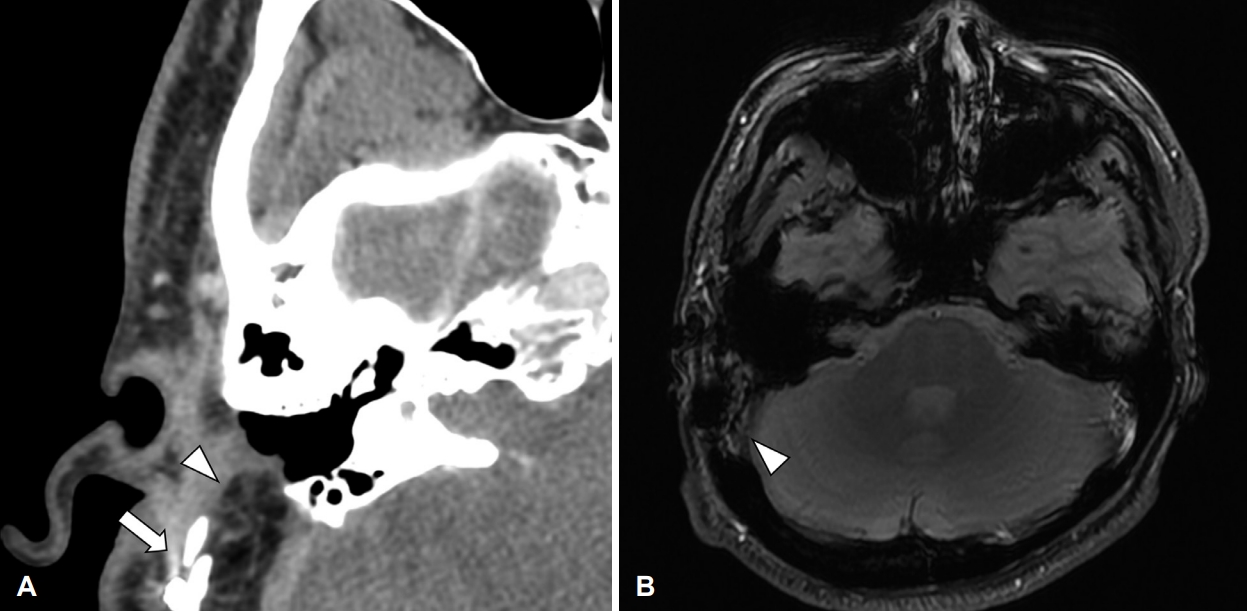
Postoperative pathologic findings revealed a lack of definite epithelium. Cholesterol cleft, focal chronic inflammation, and hemosiderin laden macrophages were identified (Fig. 4), consistent with pathologic findings indicating a cholesterol granuloma. The postoperative period was uneventful. No evidence of recurrence was observed on a temporal bone CT at three months postoperatively nor on a brain MR at six months after surgery (Fig. 5). No hearing deterioration or other surgery-associated symptoms were observed over the one-year follow-up period.
Discussion
The most common site of a cholesterol granuloma is the temporal bone, and this lesion can present in the petrous apex, middle ear, or mastoid region. Most cases of invasion into the cranial fossa are cholesterol granulomas in the petrous apex, and cranial involvement of the middle ear and mastoid region are infrequently observed [3-5]. The case discussed in this report is quite rare, as unlike in previous cases, no otologic symptoms nor middle ear involvement were observed. Conductive hearing loss can occur in patients with cholesterol granulomas in the middle ear, and cranial nerve impairment, including sensory neural hearing loss and facial palsy, can accompany cholesterol granulomas in the petrous apex [2]. Involvement of the cranial fossa may cause neurologic symptoms such as headache, insomnia, and abnormal behavior [2,3,5]. Considering the known aggressive progression of the disease, we presumed that these neurological symptoms would have occurred if the mass was left untreated. Our patient was treated prior to the onset of symptoms and recovered without complications.
Macroscopically, a cholesterol granuloma typically presents as a dark brown cyst due to hemosiderin deposition, although it can also have a yellowish color when involving adipose tissue, and demonstrates shiny properties due to cholesterol crystals [6]. Our patientŌĆÖs mass presented with typical gross findings. Martin, et al. [7] have suggested that differences in gross findings could occur between aggressive and benign cases [7], explaining that in benign cases, cholesterol-rich body fluids fill the potential space, while in aggressive cases, cysts present with thicker walls due to inflammatory reactions. Surgical findings in our patient revealed thick cystic walls similar to gross findings of previously reported aggressive cholesterol granuloma cases [8-10]. Kuruma, et al. [8] have presented several potential reasons for the aggressive expansion of certain cholesterol granulomas, indicating that negative pressure caused by drainage failure can lead to bleeding from the mucosal blood vessels and that coaptation of the marrow and mucous membranes due to exposure of the bone marrow can also lead to bleeding. In the latter case, a cholesterol granuloma from the marrow-rich petrous apex often extends into the cranial fossa. Authors also suggested a robust blood supply, such as the sigmoid sinus or carotid artery, could be a driving force for progressive cyst expansion [8,11]. In our patient, this last theory is presumed to apply to this case as the mass was found tightly adherent to the sigmoid sinus.
Oh, et al. [1] reported a case of cholesterol granuloma in the right middle cranial fossa incidentally found on a temporal CT scan following suspicion of left chronic otitis media; this patient presented with trauma history but without chronic otitis media in the right ear. This case differed from ours in that it was accompanied by conductive hearing loss on the right side, and the mass filled the epitympanum with a tegmen defect, suggesting extension from mastoid [1]. In our case, an aggressive cholesterol granuloma in the posterior fossa was found without the presence of middle ear lesions or common symptoms such as hearing loss, tinnitus, or the characteristic blue eardrum. The patient had been in a traffic accident three months before surgery that could have led to minor bleeding; this might have been a trigger of cholesterol granuloma, but there was no direct evidence that suggested the accident was the main cause of the lesion.
Complete resection of the granuloma in the middle ear is not always necessary because the purpose of treatment is to enable proper drainage and ventilation, and conservative treatment, such as insertion of a ventilation tube, can be sufficient [2]. However, cholesterol granulomas with petrous apex involvement, intracranial involvement, or aggressive tendencies usually require surgical resection. The method of surgical treatment depends on the location of the cholesterol granuloma, the hearing status of the patient, and other accompanying symptoms [2,12]. In our case, we exposed the mass via a transmastoid and suboccipital approach for complete resection, and it was removed without serious complications. In previous cases of cholesterol granuloma with intracranial involvement, some have reported re-pneumatizing the temporal bone through drainage and ventilation of the cyst [1], although some of these cases also reported cholesterol granuloma recurrence [2,3]. In most cases, complete resection of the cyst was performed [3-5,8,10,13]. Complications, such as bleeding and dura injury due to excessive dissection, can occur necessitating meticulous surgical technique. Our patient had slight bleeding due to mass adhesion to the sigmoid sinus, but resection was successful, and there were no major issues. Although surgical resection is thought to prevent recurrence, surgical methods should be selected while considering possible surgical complications.
Along with previous case reports, this paper describes the differences between a common cholesterol granuloma in the middle ear cavity and an aggressive cholesterol granuloma. Typical cholesterol granulomas are surrounded by a thin, fibrous lining, but aggressive cholesterol granulomas extending into the cranial cavity present with measurably thicker walls [1,8,10,13]. In most of these cases, adhesion to the dura or blood vessels was observed during surgery [1,4,5,8]; however, the consensus is that complications such as bleeding or dural injury can be reduced if such findings are kept in mind. Although the present patient was asymptomatic, evidence suggests that temporal bone cholesterol granulomas can cause neurological symptoms such as dizziness, headache, cranial nerve impairment, and abnormal behavior without ear symptoms. Some of the characteristics of cholesterol granulomas, including lesions of the cranial fossa, have been identified in previous cases, but more studies are needed due to their relatively rare incidence.